Background
As a result of the acute and unpredictable nature of genitourinary trauma, there is an absence of prospective, randomized controlled trials to support evaluation and management. As such, urologists have relied on case series reports, retrospective series, trauma databases from level one trauma centers, and expert opinion. Indeed, the Society of International Urology published five consensus articles pertaining to renal, urethral, bladder, ureter, and external genitalia trauma that were authored by well-respected leaders in the field of genitourinary trauma [1–5]. Each article used a level of evidence grading system to validate evaluation and management proposals: (1) supportive evidence from randomized trials, (2) supportive evidence from prospective trials, (3) supportive evidence from retrospective studies, (4) supportive evidence from case series or case reports, (5) expert opinion. Level 3 and 4 evidence predominated in each article, with occasional mention of level 1 and 2 evidence. Despite the absence of stronger levels of evidence, we strongly encourage readers to examine the articles, as they provide a wealth of information for interested urologists.
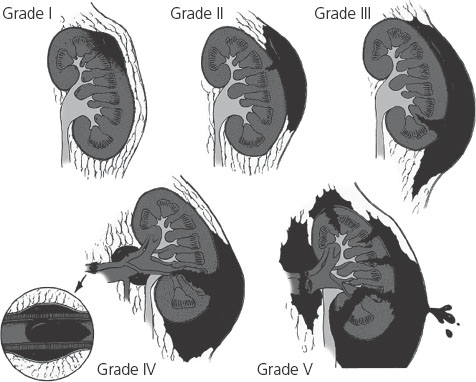
This chapter will pose two major questions from the field of genitourinary trauma that have been answered with supported evidence. References will be made to the American Association for the Surgery of Trauma (AAST) renal grading system (Figure 17.1).
Clinical question 17.1
What is the appropriate evaluation of blunt abdominal trauma in the setting of gross or microscopic hematuria?
Literature search
We searched the PubMed database for the years 1980–2008 using the search terms “blunt trauma,” “abdomen” and “hematuria.”
The evidence
The kidneys are the second most common visceral organ to be injured after blunt abdominal trauma, with most renal injuries deemed low grade. In a series of 2024 blunt trauma patients, only 81 (4%) had grade 3 or higher renal injuries [6], a finding supported by other analyses [7,8]. As such, the objective is to identify when to perform radiographic imaging for evaluation of suspected renal injury after blunt abdominal trauma.
Figure 17.1 American Association for the Surgery of Trauma (AAST) organ injury severity grade for the kidney. Reproduced from Wein et al. Campbell-Walsh Urology. Volume 2, renal and ureteral trauma, 9th edn, 2007, p. 1274, with permission from Elsevier.
Two large prospective studies have evaluated the appropriate setting of radiographic imaging after blunt abdominal trauma with gross/microscopic hematuria (Table 17.1) [6,8]. In both of these studies, blunt abdominal trauma patients were stratified into two groups: (1) gross hematuria or (2) microscopic hematuria and shock (systolic blood pressure < 90 mmHg). This classification system was based upon an earlier report from San Francisco General Hospital which found that radiographic imaging of blunt abdominal trauma patients with microscopic hematuria and no shock did not lead to complications from nonoperative management [9].
Table 17.1 Radiographic assessment of blunt abdominal trauma in the setting of gross hematuria or microhematuria and shock
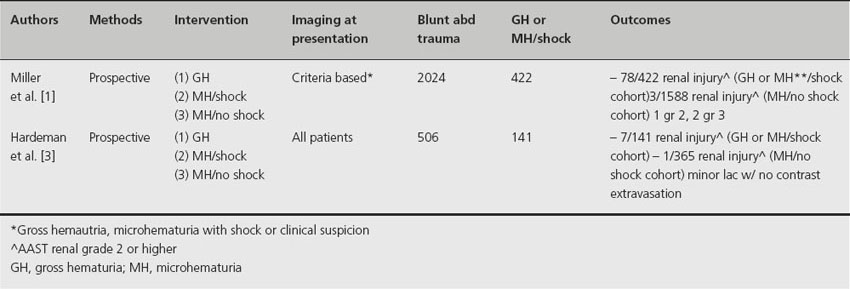
The largest series to prospectively evaluate the appropriate evaluation of blunt abdominal trauma in the setting of gross/microscopic hematuria included 2024 patients from San Francisco General Hospital [6]. This prospective series served as an update to the original series that first reported the algorithm for evaluation of blunt abdominal trauma referenced above. There were 78 significant renal injuries among the cohort of 422 patients with either gross hematuria or microhematuria and shock. Of these, there were 25 grade 2 injuries, 30 minor lacerations (grades 3–4), and 23 vascular injuries (grade 4-5). The remaining patients (344) had renal contusions (grade 1 injury). Only 3/1588 patients with microhematuria and no shock were found to have significant renal injury (grade 2 or higher). Two of these injuries (one grade 2 and one grade 3) were discovered after imaging for suspected intra-abdominal injury, while the third injury (grade 3) was discovered at the time of exploratory laparotomy for associated intra-abdominal injuries. Therefore, urologists are encouraged to perform abdominal imaging if there is suspected renal trauma even in the absence of shock or hematuria.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


