Gastric Neoplasms
Most neoplasms of the stomach are malignant, and most of those are adenocarcinoma. A minority are lymphoma, leiomyosarcoma, and liposarcoma. Benign neoplasms include adenomatous, hyperplastic, and hamartomatous polyps; leiomyomas; and lipomas. Rarely, gastrinomas, carcinoids, vascular tumors, fibromas, and squamous cell carcinomas occur in the stomach.
Adenocarcinoma of the stomach is the second most frequent cause of cancer death worldwide. In East Asia, Latin America, and the former Soviet Union, the incidence is up to eight times higher than in the United States and it remains high among immigrants from those areas. Although screening programs in high-risk areas such as Japan may result in the detection of early lesions, in lower risk areas such as the United States and Western Europe, most cancers are relatively advanced by the time of diagnosis.
I. GASTRIC ADENOCARCINOMA
A. Pathogenesis
1. Pathology
a. Early gastric cancer (EGC) is gastric cancer that has not penetrated the major muscle layer of the stomach wall. EGC can be divided into three types based on macroscopic appearance (Fig. 27-1).
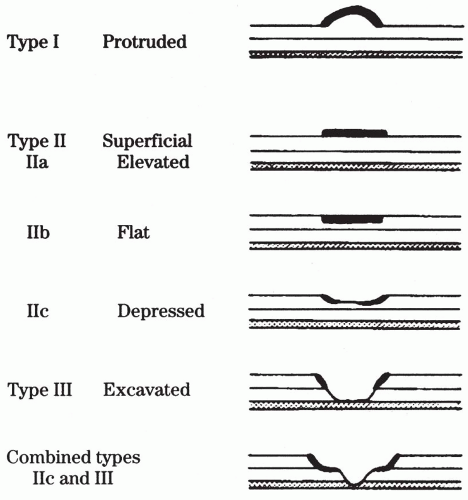 Figure 27-1. Classification of early gastric carcinoma according to the Japanese Endoscopy Society. (From Green PHR, et al. Early gastric cancer. Gastroenterology. 81;247:1981. Reprinted with permission.) |
b. Advanced gastric cancer is gastric cancer that has penetrated the muscle layer of the stomach. This condition also has been divided into three types:
i. Polypoid or intestinal
ii. Diffuse infiltrating or signet ring type
iii. Ulcerating
2. Risk factors
a. Some population groups appear to be at higher risk than others for development of gastric adenocarcinoma. For example, the prevalence of gastric cancer in Japan is about 10 times the prevalence in the United States. Furthermore, in Japan approximately 30% of gastric cancers at the time of diagnosis are EGC, whereas in the United States only 5% can be classified as EGC. Japanese who move away from Japan to a low-risk area have a similar risk to those who remain in Japan. However, second- and third-generation Japanese children of these immigrants have a progressively lower risk that approaches the local population.
b. Several dietary factors have been implicated. Increased consumption of salt appears to be a consistent finding. Dietary nitrates also may be important. Cigarette smoking increases risk. However, a diet rich in fresh fruits and vegetables, daily aspirin use, and COX-II antagonist reduce the risk.
c. Conditions that predispose to achlorhydria, such as pernicious anemia and atrophic gastritis, carry a higher than average risk of gastric cancer. Whether this is because the reduced acid allows bacteria that have the capacity to nitrosate dietary amines to carcinogenic nitrosamines to grow within the stomach or because of other effects is not clear.
d. Partial gastrectomy 15 or more years in the past was thought to be associated with a higher risk of development of adenocarcinoma within the gastric remnant. Recent evidence indicates that this increased risk is lower than originally anticipated. Virtually all these patients eventually have chronic gastritis and become hypo- or achlorhydric, which, as indicated previously, may increase the risk of development of cancer.
e. Helicobacter pylori infection has been associated with gastric adenocarcinoma. The cancer is thought to arise from gastric intestinal metaplasia that arises in patients who develop chronic atrophic gastritis with chronic infection with H. pylori. Especially those strains that are CagA+ appear to be more carcinogenic than CagA− strains.
B. Diagnosis
1. Clinical presentation
a. EGC typically is asymptomatic and usually is discovered during endoscopy performed for other complaints. When symptoms have been attributed to EGC, they usually are vague, such as epigastric discomfort and nausea.
TABLE 27-1 Risk Factors for Adenocarcinoma of the Stomach | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
b. Most patients in North America present with symptoms of advanced gastric cancer.
i. Symptoms are primarily abdominal pain and weight loss, which may be accompanied by anorexia, weakness, gastrointestinal bleeding, and signs of gastric obstruction, such as early satiety or vomiting.
ii. Physical examination.




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
