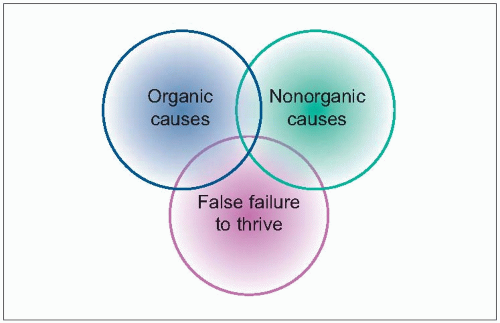
FTT is a clinical label frequently used to describe infants and young children, generally under 3 years, who fail to grow as expected using established growth standards for age and gender along a period of time (usually longer than 3 months) (
1.1).
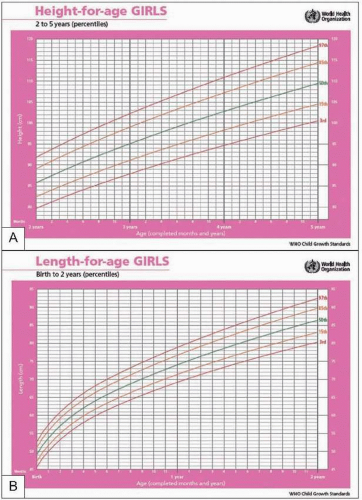
Weight is a measure of the varying combination of height, body fat, and muscle bulk, which makes it a less straightforward measure of growth than height. Nevertheless, because of its widespread availability and ease of measurement, it is the most usual tool when growth measure is considered. What constitutes a normal rate of weight gain (
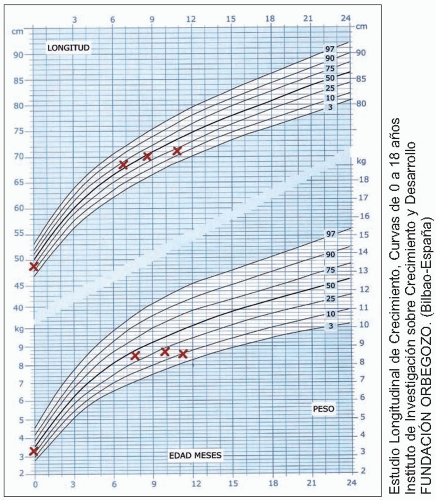
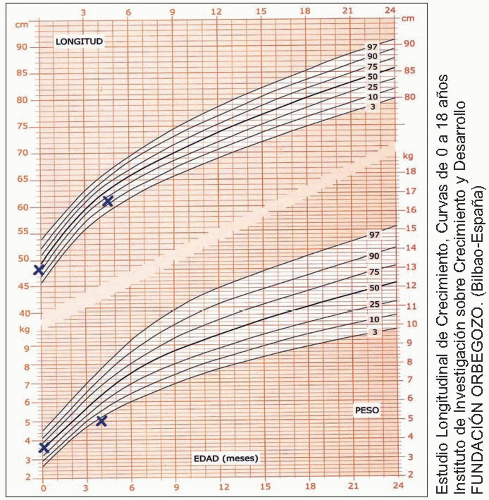
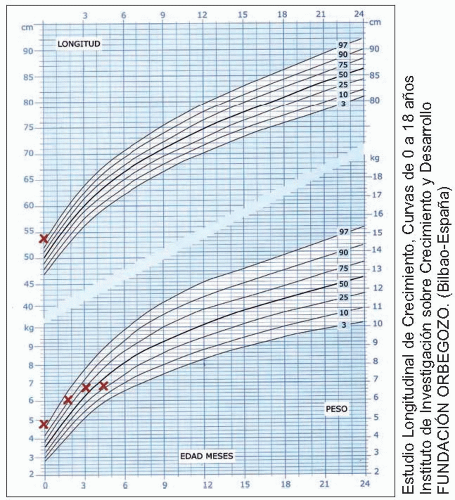
Table 1.1)? It is often assumed that normal growth constitutes tracking along the birth centile. However, weight at birth is a reflection of the intrauterine environment and is of limited prognostic value. Many children deviate from their earlier centile position, and this divergence may not become pathological. Although the most commonly used definition of abnormality is that falling below a predetermined centile, usually the third (
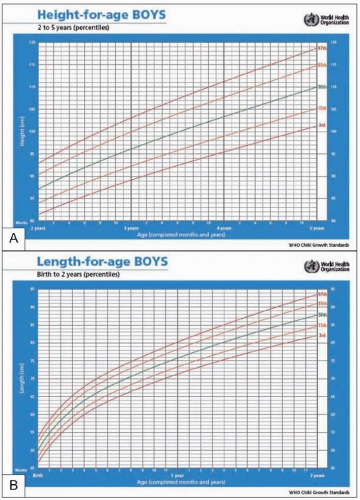
1.2), this would include a number of constitutionally small children. An alternative definition applies when a child has a weight curve that has fallen more than two standard deviations or
percentiles below a previously established rate of growth. However, up to 30% of healthy term infants cross one percentile line and 23% cross two percentile lines (in either direction) by the age of 2 years.