(1)
Gastroenterology and hepatology, Chinese PLA General Hospital, Beijing, China, People’s Republic
Abstract
In this chapter we described the experimental researches in porcine models of tunnel technique for mucosal lesions, for resection of muscularis propria, for myotomy of muscularis propria, researches of tunnel technique into the mediastinum and researches of percutaneous tunnel technique for mediastinal lesions.
10.1 Experimental Researches of Tunnel Technique for Mucosal Lesions
Now, ESD has become a standard technique for the dissection of esophageal neoplasia and early cancer [1, 2]. The procedure of classic ESD is as follows: marking the margin of the lesion, submucosal injection to form liquid cushion, annular mucosal incision, submucosal dissection along the margin. However, with respect to large-size esophageal lesions, especially for lesions >2.5 cm, the mucosal lifting by submucosal injection was not as good as before, which made the dissection slow down, the incidence of complications such as perforation was also increased. In 2009 we established the peroral tunnel technique successfully to dissect esophageal circumferential lesions, so we wonder whether tunnel technique can be used for more than 2.5 cm esophageal submucosal lesions dissection, and whether this technique can speed up the dissection process or reduce the incidence of complications. Therefore, on Jan of 2011, we carried out the animal experimental study on endoscopic dissection of large-size esophageal lesions with submucosal tunnel technique in porcine model.
10.1.1 Materials and Methods
10.1.1.1 Experimental Animals
All the six 4-month old domestic swine were female, with weight 23–38 kg, as shown in Table 10.1.
Table 10.1
Guinea pig general conditions
Sex | Weight (kg) | |
|---|---|---|
1 | F | 23 |
2 | F | 27 |
3 | F | 28 |
4 | F | 38 |
5 | F | 25 |
6 | F | 31 |
10.1.1.2 Instruments and Accessories
Q260J endoscopy (Olympus); ICC-200 high-frequency electrogenerator (ERBE); injection needle, needle knife, IT2 knife, hook knife, Dual knife (Olympus); snare, transparent cap, hemostatic clips.
10.1.1.3 Methods
Preparations Before Surgery
Pigs were fasted 72 h before the procedure and water was also fasted 12 h before. The procedures were done under general anesthesia with endotracheal intubation for ventilator-assisted breathing. The anaesthetist monitored the porcine vital signs, including blood pressure, heart rhythm and oxygen level.
Operation Methods
1.
Conventional endoscopy, cleaning the esophagus, to assess the esophageal available length;
2.
Location of mucosae to dissect: 44 cm or 30–42 cm proximal to incisors.
3.
The length of dissected mucosae is from 8 to 10 cm, and the width of that is approximately half the lumen perimeter;
5.
Submucosal injection (Fig. 10.1b): A submucosal lift is performed by injecting glycerol and fructose solution at designated cut point.
6.
Cut the distal edge of the lesion (Fig. 10.1c1, c2): The elevated mucosa of the distal edge of the lesion is incised transversely for 1–1.5 cm until reaching submucosa;
8.
Establish the tunnel: ESD was used to create a submucosal tunnel downwards from the proximal incision until reaching the distal incision (Fig. 10.1e);
9.
Dissection of the lateral edge of the lesion was performed from the anal side along the margin of the marked lesion with a IT knife until the lesion was completely dissected (Fig. 10.1f, g);
10.
The lesion was then removed and the potential bleeding area in the tunnel was coagulated to prevent delayed bleeding.
10.1.2 Results
10.1.2.1 Lesions Removes and the Procedure Time (See Table 10.2)
Table 10.2
Size of removed lesions and the procedure time
Remove mucosa size (cm) | Time-taken (min) | |
|---|---|---|
1 (27 kg) | 10 | 100 |
2 (27 kg) | 8 | 50 |
3 (23 kg) | 10 | 55 |
4 (23 kg) | 8 | 46 |
5 (28 kg) | 9 | 70 |
6 (28 kg) | 8 | 50 |
7 (38 kg) | 10 | 90 |
8 (25 kg) | 10 | 60 |
9 (25 kg) | 8 | 45 |
10 (31 kg) | 9 | 55 |
Ten simulated lesions in six pigs had a mean length of 9.0 cm (range 8–10 cm) and had a width of half the lumen perimeter (Fig. 10.1h). The mean procedure time was 62 min with a range of 45–100 min.
10.1.2.2 Complications
Complete dissection of ten lesions was achieved in all pigs with no complications as perforation and bleeding.
10.1.3 Discussions
Submucosal tunnel technique is to create a channel between the mucosal layer and the muscularis propria layer endoscopically. Diagnostic and therapeutic endoscopy could be performed through the channel, such as doing endoscopic treatment to the mucosal side or the muscularis propria side or outside of the gastrointestinal lumen. On May of 2009, we had successfully applied submucosal tunnel technique for dissecting long circumferential esophageal lesions. At the same time, Yoshizumi also reported the approach to build a submucosal tunnel with ESD technique as a operation pathway of NOTES in porcine mode [3].
We are the first team to clinically use the peroral tunnel technique to remove esophageal mucosal lesions greater than 2.5 cm in diameter. The use of the technology aimed to speed up the submucosal dissection in esophageal precancerous lesions and early cancers and the outcomes of the present study are promising.
First of all, by animal experiments, we found that simulated lesions more than 2.5 cm in diameter can be separated by tunnel technique, and there was no excessive esophageal mucosa that had been removed by this technique. Then, what is the minimum size to employ submucosal tunneling technique? The diameter of the endoscope attached with a transparent distal cap is 1 cm, and thus the circumference of the narrowest tunnel should be 3.14 cm (1 × 3.14 cm). And therefore, it is theoretically possible for lesions larger than 1.6 cm in diameter (3.14/2 = 1.57) to adopt the technique. The normal esophageal diameter is approximately up to 2 cm. Lesions of 1/3 of the esophageal circumference over 2 cm in diameter (2 cm × 3.14/3 = 2.09 cm), which can be completely dissected by submucosal tunnel technique.
There are two significant advantages for incision of the distal margin of the lesion before creating the tunnel. First, the distal incision facilitates determining the targeted end of the tunnel. Then, the distal incision prevents excessive gas collection within the tunnel, which may result into excessive mucosa separation. In our pilot study when incision of the distal margin was not performed before tunnel establishment, excessive separation had been found in one pig, which is yet effectively avoided by application of the “distal incision first” principle.
Distinguishment of the margins of the lesion during the process of dissection: the process of endoscopic tunnel establishment is also the process of dissection. We can see the designated marker on the mucosa, then we can decide the direction and the affected proportion during the submucosal tunnel establishment. And meanwhile, the scope can go in and out of the tunnel to check the situation of dissection and correct the tunnel direction.
The tunnel technique can really speed up the mucosal dissection: this research dissected 8–10 cm long lesions in an average of 62 min, significantly shorter than the general duration of the ESD in human body, because the lasting existence of submucosal space makes it easier and more convenient to finish those endoscopic operation, such as blunt dissection, electric coagulation and electrotomy.
The dissection of the edge of the lesions is different from the classic ESD, which raises high requirement for precise submucosal injection prior to dissection. As for tunnel technique, we just need to use IT knife for resection of the lateral margins of the lesion after tunnel establishment.
At the same time, submucosal tunnel technique changes the routine procedure of ESD, which replaces the steps from submucosal injection-mark-circle incision-dissection to submucosal injection-mark-distal incision-proximal incision-establishing submucosal tunnel-dissection of the lateral margin.
Through animal researches [4], we concluded that tunnel technique is a safe, effective and time saving method to dissect esophageal large-size lesions. It also prevents complications such as gastrointestinal tract leakage and secondary infection of chest and abdominal cavity. Nevertheless, further clinical research is necessary to clarify its safety and efficacy in humans.
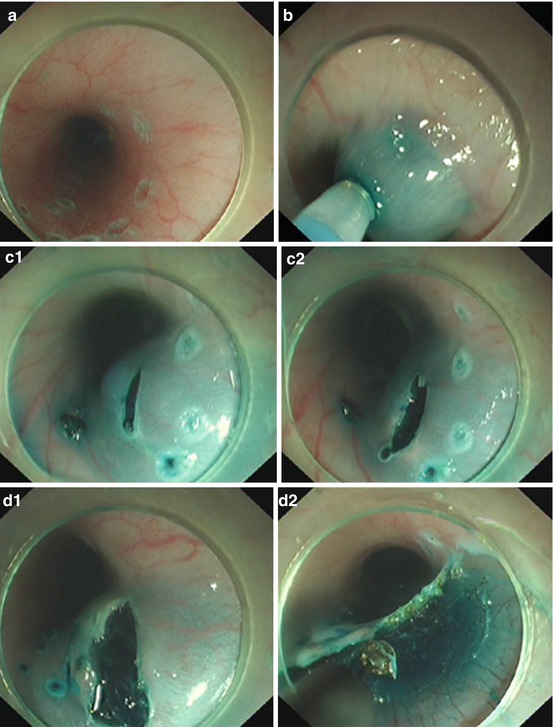
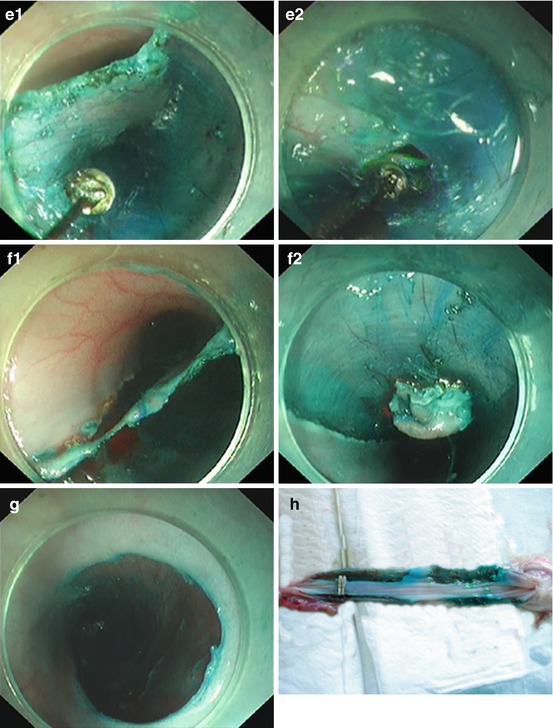
Fig. 10.1
(a) Marking the margin. (b) Submucosal injection. (c1) Distal incision. (c2) Distal incision. (d1) Proximal incision. (d2) Proximal incision. (e1) Establishing a tunnel. (e2) Tunnel extend downward till the distal incision. (f1) Lateral dissection. (f2) Lesion retracted after almost complete dissection. (g) Mucosal defect after dissection. (h) Resected mucosal lesion
10.2 Experimental Researches of Tunnel Technique for Resection of Muscularis Propria
SMTs from muscularis propria could be treated either by surgery or endoscopy, yet esophageal perforation after treatment could cause a serious outcome like pneumothorax. If a minimally invasive endoscopic treat could well prevent the complication of pneumothorax, then it would benefit patients greatly considering the invasiveness of surgery. After we firstly used peroral tunnel technique to treat esophageal mucosal lesions we then though of the possibility of using this new technique to perform resection of muscularis propria tumors in the procedure of making oral incision-establishing submucosal tunnel-resecting the tumor-sealing the incision of the tunnel. And this assumed procedure might well prevent perforation and thus we perform peroral resection of esophageal muscularis propria in porcine model by tunnel technique [5].
10.2.1 Methods
10.2.1.1 Animals
All the two 4-month domestic swine were female, with weight of 30 and 32 kg.
10.2.1.3 Anesthesia
The operation was done under general anesthesia. Animal Narcotic Drugs is Sumianxin No. II (formerly known as 846 agents), composed of the hydrochloric acid dihydroetorphine, haloperidol, Baoding Ning, 0.3 ml/kg body weight (1.5 ml/support); succinylcholine chloride 0.1 mg/kg · min, diazepam 0.2 mg/kg · min. During the surgery, a mixed solution of methylene blue and saline was used for submucosal injection.
10.2.1.4 Operator
An endoscopist with ESD experiences
10.2.1.5 Procedure
1.
Conventional endoscopy, cleaning the esophagus;
2.
Determine the incision position of tunnel: 30 and 40 cm to the incisor teeth;
4.
Establish a tunnel of 8-cm in length;
6.
Resection of muscularis propria: expose the muscularis propria and use the triangular knife to incise the circular muscle and longitudinal muscle layer by layer, and then perform circular incision;
8.
Coagulation of the blood vessel to prevent bleeding;
10.
Performing a chest radiograph for pneumothorax.
10.2.2 Results
Operations were successfully completed in both pigs. The resection of muscularis propria required 40 and 50 min. No hemorrhage occurred. The wound diameter was 1 cm and the mediastinal fat was visible during operation; Left pneumothorax and right pneumothorax happened respectively in both pigs, and disappeared after 100 and 20 ml of aspiration by syringe. Kept fasted with intravenous liquid supply for 48 h after surgery, both pigs survived well.
Related posts:
 Indications of Tunnel Technique
Indications of Tunnel Technique
 Principle of Digestive Endoscopic Tunnel Technique
Principle of Digestive Endoscopic Tunnel Technique
 Tunnel Technique for SMTs Originating from Muscularis Propria
Tunnel Technique for SMTs Originating from Muscularis Propria
 Tunnel Technique for Digestive Mucosal Lesions
Tunnel Technique for Digestive Mucosal Lesions
 Techniques in Tunnel Establishment
Techniques in Tunnel Establishment
 Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


