Anatomy
Papilla intact?
Short afferent limb
Bilroth II gastrojejunostomy
Yes
Long afferent limb
Whipple’s procedure
No
Gastrojejunostomy
Yes
Choledochojejunostomy/hepaticojejunostomy
No
Total gastrectomy with esophagojejunostomy
Yes
Very long afferent limb
Gastric bypass
Yes
Biliary diversion “duodenal switch”
Yes
Short afferent limbs are most commonly encountered in patients following a Billroth II gastrojejunostomy, as the afferent limb is anastomosed directly to the gastric remnant. In patients with retrocolic Billroth II anastomosis, the length of bowel that must be traversed can be as short as 30 cm [5]. These limbs can be traversed with a duodenoscope, though at times the acute angulation at the anastomosis may require a more flexible forward viewing endoscope or balloon-assisted enteroscopy (BAE) [5, 6]. The use of a side viewing duodenoscope has also been reported for patients with a gastrojejunostomy or pylorus-preserving Whipple procedure [6], though this mandates both a short afferent limb and an easy-to-navigate anastomosis.
More commonly, patients with a longer afferent limb such as those patients who have undergone a “standard” Whipple procedure or those with a Roux-en-Y anastomosis require the use of a long forward viewing endoscope or enteroscope [6, 7]. The lengths of Roux limbs are variable. Short afferent limbs (<50 cm) are commonly encountered in patients with oncologic, transplant, or biliary-diverting procedures such as total gastrectomy with Roux-en-Y esophagojejunostomy, Roux-en-Y choledochojejunostomy, or hepaticojejunostomy [8]. These limbs will have variable papillary anatomy depending on the original indication for surgery (see Table 15.1). Bariatric surgery typically results in a long Roux limb (>100 cm) to promote malabsorption as well as prevent bile reflux [9]. These longer limbs may require the use of overtube-assisted devices for deep enteroscopy, such as BAE or rotational enteroscopy (RE). In addition to particularly long and tortuous Roux limbs, patients who have undergone a Roux-en-Y gastric bypass have a remnant stomach. This can allow for an additional access point (surgical gastrostomy, endoscopic-assisted gastrostomy) for performing ERCP. For the rare patient who has undergone pancreatico-biliary diversion (“duodenal switch”) for obesity, the Roux-en-Y anastomosis can, in some cases, be reached with difficulty using the retrograde approach with BAE [5]. As with Billroth II anatomy, patients with gastric bypass or pancreatico-biliary diversion will generally have native papillary anatomy.
Technical Aspects of ERCP in the Surgically Altered Anatomy
There are three significant challenges to successful ERCP in altered anatomy: reaching the papilla or pancreatico-biliary anastomosis (enteroscopic success), identification and cannulation of the papilla or pancreatico-biliary anastomosis (diagnostic success), and finally, performing therapy if indicated (therapeutic success). A learning curve for successfully performing each of these three maneuvers has been described [10], and, although no single standardized approach exists, there are certain techniques which, when employed, can optimize the chances of overall endoscopic success.
Enteroscopic Success
Preprocedure Planning
With considerable variability in postsurgical anatomy, preprocedure planning is essential. When adequately prepared, the endoscopist can decrease the procedure duration, select the appropriate endoscope, and have the appropriate tools available at the time of endoscopy. Most importantly, the previous operative report should be obtained, recent cross-sectional imaging reviewed, and if possible, a discussion with the surgeon who performed the original operation [11]. Depending on operator expertise and difficulty of the procedure, the range of times reported for ERCP in altered anatomy can vary from 24 to 150 min [12–14]. The increased complexity and longer procedure duration in patients with postsurgical anatomy may necessitate the use of an anesthesiologist, as adequate (and safe) sedation almost certainly plays a role in affecting the procedure outcome. Several groups have reported improved intubation depth, patient comfort, and decreased overall procedure duration with the use of CO2 for procedures employing BAE [15, 16].
In patients with short afferent limbs, such as those with Billroth II gastrojejunostomy, a duodenoscope may suffice and provides the benefit of both an elevator and availability of standard ERCP tools. In patients with longer limbs, success has been reported with either the 164 cm long pediatric colonoscope or 240 mm long “standard” enteroscope [7, 17] both with and without the assistance of a gastric overtube. Gastric overtubes may reduce looping in the stomach and duodenum; in patients who have undergone gastrectomy, gastric overtubes are rarely needed. If a colonoscope is used, it is preferable to use one with a variable stiffness setting. Initial insertion is performed on the most flexible setting and the stiffness is increased once the endoscope is passed into the small intestine to reduce loop formation. In patients with longer intestinal limbs, it may be necessary to use the “hook and pull” technique to advance the endoscope deeper into the small intestine. The use of a colonoscope to place a wire into the pancreatico-biliary limb in patients with Roux-en-Y anatomy followed by advancement of a duodenoscope over the wire has been described [17]. More recently the advent of overtube-assisted enteroscopy (both BAE and RE) has allowed the endoscopist a means to navigate tight angulation at the anastomosis and very long Roux limbs to access the pancreatico-biliary tree.
Overtube-Assisted Enteroscopy
Several techniques are now available to perform overtube-assisted deep enteroscopy including the double balloon enteroscopy (DBE), single balloon enteroscope (SBE), and RE. In general, RE and balloon-assisted enteroscopy (BAE) consist of a forward viewing enteroscope that travels through a flexible overtube. As such, overtube-assisted enteroscopy is a term that can encompass both RE and BAE. RE utilizes a rotating overtube that sequentially reduces and pleats the small bowel over a standard enteroscope. In the case of BAE, there is either a balloon on the distal tip of the overtube (single balloon) or a balloon on both the overtube and the distal tip of the enteroscope (double balloon). The operator is able to inflate or deflate the balloons selectively. Using a push-pull technique, BAE works by pleating the bowel over the endoscope as it is advanced, using balloons to stabilize the device for both forward progress and reduction. With a double balloon, the endoscope is advanced and the balloon at the tip of the endoscope is then inflated, anchoring the scope tip. The overtube is then advanced over the endoscope and, once the overtube has reached the end of the scope, the overtube is inflated and either reduction can be performed or the endoscope balloon can be deflated and advanced further. The single balloon technology works in the same fashion, though without a balloon over the endoscope tip. This sacrifices a degree of stability but provides added flexibility, faster set-up time, and decreased complexity of balloon coordination [18].
Several authors have reported conceptualizing the overtube as a “large working channel” to assist ERCP [19–21]. Once the enteroscope is advanced to the ampulla or the pancreatic or biliary anastomosis, the balloon is inflated on the overtube and reduction is performed. This anchors the overtube and the enteroscope is then removed. In the case of longer overtubes, an incision can be made in the overtube just outside of the patient (taking care not to damage the balloon air channel) and a gastroscope or ultraslim gastroscope can be advanced to the ampulla. This allows passage of standard-biliary tools such as stents [20] that are precluded by the long and narrow working channel of the enteroscope, or direct cholangioscopy [21, 22].
Afferent Limb Intubation
Regardless of anatomy, selecting the appropriate limb to traverse can be the first challenge reached by the endoscopist. Selecting the wrong limb adds time to an already lengthy procedure. In general, the endoscopist will encounter two or three potential lumens (Fig. 15.1) at the surgical anastomosis. If three lumens are visualized, invariably one of the openings is not a true opening, rather a “blind end,” created by the end-to-side creation of the anastomosis. The passage visualized directly adjacent to this lumen is usually the efferent limb. Between these openings one should not see a surgical scar. If the efferent limb is entered and traversed for some distance the endoscopist will generally see multiple loops forming on fluoroscopy. Bile is not a reliable marker to indicate the afferent limb, though generally a greater amount of bile is found in the afferent limb. One group has reported improved identification of the afferent limb in patients with Roux-en-Y anatomy by injecting indigo carmine just beyond the stomach or the esophagojejunostomy. When the anastomosis is then reached, the afferent limb reportedly took up less indigo carmine and thus decreased time of procedure with little added expense or technical challenge [23].
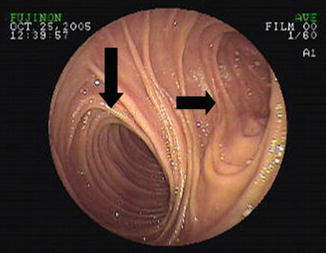
Fig. 15.1
Endoscopic image demonstrating the typical appearance of a jejunojejunostomy in a patient following a Roux-en-Y gastric bypass. The vertical arrow points to the typical location of the efferent limb whereas the horizontal arrow demonstrates the blind limb. The pancreatico-biliary limb cannot be seen in this image
It is not uncommon for endoscopists to become disoriented at the site of the anastomosis and, after accidentally traversing the efferent limb, reintubate the incorrect lumen. Once the appropriate limb has been determined, several groups advocate tattooing the afferent limb for improving ease of future access [24, 25]. Others recommend tattooing the limb that is initially intubated to prevent reintubation if this becomes the incorrect limb [26]. In either circumstance, clear documentation of which limb was tattooed is essential to expedite future endoscopy.
The second challenge to successful afferent limb intubation is navigating an often acute angulation. The afferent limb is generally located at 5–8 o’clock and should take off at a right angle—essentially an almost 180° turn once the endoscope is inserted into the Roux-en-Y anastomosis. If a variable stiffness colonoscope is used, making this turn should be attempted using the most flexible setting. Occasionally, changing the patient’s position to left lateral decubitus or applying abdominal pressure can help navigate the turn. Fluoroscopy often can help confirm passage in the proper direction. If BAE systems are used, it is useful to reduce the scope as much as possible once the jejuno-jejunal anastomosis is reached (in the case of a Roux-en-Y anastomosis). Following reduction, the tip of the endoscope is advanced as deep as possible into the pancreatico-biliary limb. The balloon at the tip of the endoscope is then inflated and the endoscope tip is “hooked” into the limb using a combination of tip deflection and suction while the overtube is advanced through the anastomosis and into the pancreatico-biliary limb [5]. Despite these maneuvers, further advancement can be impossible. In these instances, a wire can be advanced downstream under fluoroscopy and a large balloon advanced over the wire. Using this balloon as an anchor, the enteroscope can be slowly inched forward [27].
Diagnostic Success
Once the proximal aspect of the pancreatico-biliary limb is reached, the next challenge lies in identifying the papilla, pancreatic, or biliary anastomosis and obtaining deep cannulation with the forward viewing endoscope. It is during cannulation and consideration of therapy that the lack of ERCP-specific tools, lack of an elevator, the altered vector forces, and abnormal anatomy (inverted orientation of the papilla) provide the greatest difficulty to providers accustomed to performing standard ERCP with a duodenoscope.
In patients with a choledochojejunostomy, hepaticojejunostomy, or pancreaticojejunostomy, cannulation is often relatively easy if the anastomosis can be found. Due to their small nature, the anastomosis may be difficult to find, either secondary to near complete stenosis or due to the positioning of intestinal folds or anatomic turns in the bowel (Fig. 15.2a). The hepaticojejunostomy is generally located 10–15 cm downstream from the blind end and is typically found in the lower left field of view. Administration of intravenous sincalide (Kinevac, Bracco Diagnostics, Princeton, New Jersey) at a dose of 0.02 μg/kg can be performed to stimulate the secretion of bile allowing identification of the biliary anastomosis. In patients with pancreaticojejunostomy, secretin (SecreFlo, Chesapeake Biologic Labs, Baltimore, Maryland) administered intravenously as a 0.2 μg/kg bolus can helpin a similar fashion. The use of a clear plastic cap (Olympus Co LTD, Japan) affixed to the tip of the endoscope can help improve visualization of bilio-digestive anastomoses, as well as aid the visualization and cannulation of native papillae [19, 25]. The cap may also help anchor the endoscope during reduction via mucosal suctioning [12, 28]. Once found, cannulation is often amenable to forward viewing cannulation from the 6 o’clock accessory channel [18].
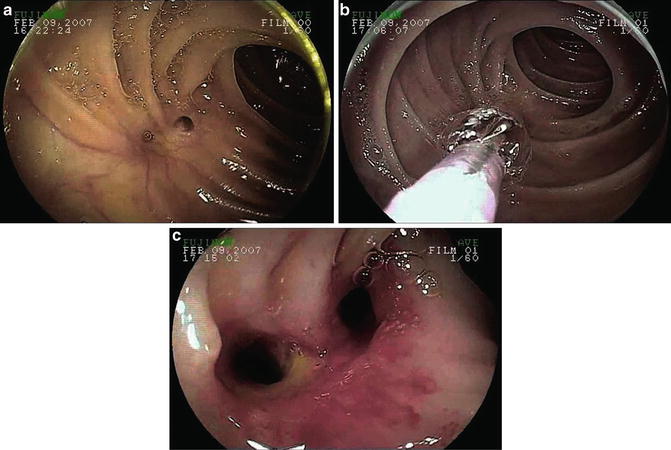
Fig. 15.2
(a) Typical endoscopic appearance of a hepaticojejunostomy. Note that the anastomosis is stenotic. (b) Balloon dilation of the hepaticojejunostomy using a controlled radial expansion balloon. (c) Postdilation appearance of the hepaticojejunostomy
In patients with an intact “native” major papilla, a forward viewing endoscope will generally find the ampulla located at the 6 o’clock position [18] and “inverted.” Cannulation of both native and anastomotic lumens is typically performed using a straight single or double lumen catheter after achieving wire guided access. The use of a clear plastic hood affixed to the endoscope tip may be useful in identification and cannulation of the native papilla. As with standard ERCP, in some instances where papillary anatomy preferentially results in pancreatic duct cannulation, biliary cannulation can be assisted by pancreatic duct stent placement and wire guided cannulation over the pancreatic duct stent (Fig. 15.3).
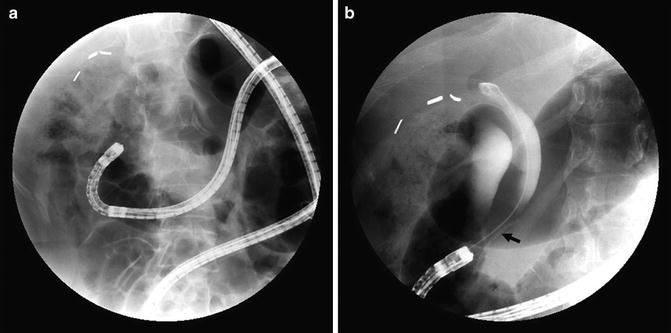
Fig. 15.3
ERCP performed using a double balloon enteroscope in a patient following RYGB. Note that biliary cannulation was achieved over a pancreatic duct stent (arrow)
Therapeutic Success
After successful cannulation, the final step is delivery of therapy, often dilation of an anastomotic stricture, stone removal, bleeding treatment, or stent placement (demonstrated in Figs. 15.4, 15.5, and 15.6.). Forward viewing equipment provides the following challenges: lack of an elevator making wire exchanges tenuous, small diameter of working channel (generally a 2.8 mm channel compared to 4.2 mm standard duodenoscopes), and an increased length of the working channel precluding many standard ERCP tools. Lastly, due to the length of the scope, the small diameter of the working channel, and the often multiple loops of the endoscope, there can be considerable resistance to wire and accessory passage. This last point can be improved with the use of a lubricant placed on the tip of the wire before advancement—either silicone or a spray oil such as PAM (ConAgra foods, Omaha, Nebraska). A review of available scope length and working channel diameters is provided in Table 15.2 (tools).
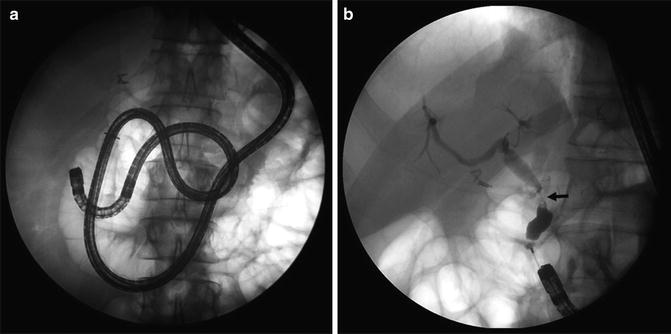
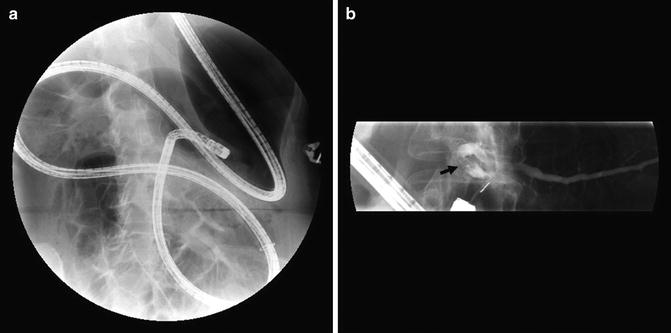

Fig. 15.4
ERCP performed following a Roux-en-Y esophagojejunostomy in a patient status post total gastrectomy for gastric cancer. Note the presence of a high-grade mid-common bile duct stricture (arrow)
Fig. 15.5
ERCP performed in a patient following a central pancreactectomy with a Roux-en-Y pancreaticojejunostomy. Note the presence of a large pancreatic duct stone (arrow).
Fig. 15.6
Cholangiogram demonstrating a high-grade stricture of the common hepatic duct in a patient following a Whipple procedure for a cholangiocarcinoma of the distal common bile duct
Table 15.2
Endoscopes used in altered anatomy
Endoscopes | Working channel (mm) | Working length (cm) | Distal end diameter (mm) | Overtube | Diameter (mm) | Length (cm) |
|---|---|---|---|---|---|---|
Balloon-assisted endoscopes | ||||||
EN-450T5, Fujinon | 2.8 | 200 | 9.4 | TS-12140 | 13.2 | 145 |
EN-450P5, Fujinon | 2.2 | 200 | 8.5 | TS-12140 | 12.2 | 145 |
EC-450B15, EI-530B, Fujinon | 2.8 | 152 | 9.4 | TS-13101 | 13.2 | 105 |
SIF Q180, Olympus | 2.8 | 200 | 9.2 | ST-SB-1 | 13.2 | 140 |
SIF Q160Y, Olympus | 2.8 | 200 | 8.4 | ST-SB-1 | ||
SIF-Y0004, Olympus | 3.2 | 152 | 9.2 | NR | NR | 88 |
Spiral endoscopes | ||||||
Endo-Ease Discovery SB (DSB), Spirus | NAa | 17.5 | 130 | |||
Sphincterotomy is typically performed by placement of a stent into either the pancreatic or bile duct followed by needle knife sphincterotomy over the stent (Fig. 15.7). Rotatable sphincterotomes have been reported [25] and some have reported success with limited sphincterotomy followed by controlled radial expansion (CRE) balloon dilation [19]. In general, the performance of other therapeutic maneuvers is relatively straightforward given the previously listed limitations. It should be noted that due to the long length of accessories, the assistant may “lose” the wire during exchange due to increased length relative to the wire guide being used. Whenever possible, the longest wire guide available should be used. If wire is “lost,” use of a 60 mL syringe filled with water or saline affixed to the accessory in the process of exchanging can be used to create a static column of water. This, along with gentle counter pressure, can help avoid losing duct access.
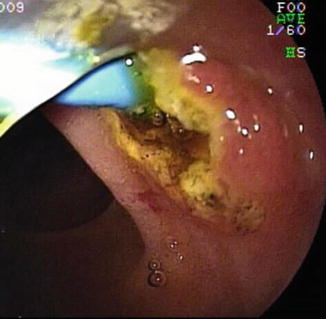
Fig. 15.7
Endoscopic image showing a needle knife biliary sphincterotomy performed over an indwelling pancreatic duct stent. Notice the direction of the cut is toward the 4 o’clock position on the inverted papilla
With the small diameter (2.8 mm) of most enteroscope or colonoscope working channels, a 7 Fr plastic stent is the largest caliber plastic endoprosthesis that can be used. Additional equipment such as enteroscopy-length sphincterotomes, needle knife, and extraction balloons and baskets are available. For balloon dilation, many have reported success using colonic length-CRE dilation balloons [18, 19] (Fig. 15.2b, c). A shorter double balloon enteroscope with a 2.8 mm working channel and 152 cm working length is available from Fujinon and an Olympus prototype has been reported with a 3.2 mm working channel and 150 cm working length. These endoscopes allow the use of shorter wires and standard ERCP implements, though they are still limited in working channel diameter size. As a workaround, several groups have reported using the overtube as a large working channel. Once the overtube is advanced to the pancreatico-biliary limb, anchored with balloon inflated, and wire guided cannulation is achieved, the endoscope is exchanged out leaving the wire or a long balloon inflated in the bile duct. A hole is cut in the overtube just outside the patient’s mouth and shorter instruments such as self-expanding metal stents (SEMS) or ultraslim gastroscopes for direct cholangioscopy can then be utilized [12, 21, 22].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


