The epidemiology of esophageal cancer has radically changed in the last fifty-years in the Western world. Changes in the predominant type of squamous cell carcinoma to adenocarcinoma, disparities between different ethnicities, and the exponential increase in incidence rates of adenocarcinoma have established esophageal cancer as a major public health problem requiring urgent attention.
The epidemiology of esophageal cancer is fascinating, yet remains very poorly understood. Advances in data collection and surveillance, not to mention the development of national cancer registries to collect incidence data in developed and developing countries, have provided more accurate monitoring of this disease over the last few decades. Currently, esophageal cancer is the eighth most common incident cancer in the world and, because of its extremely aggressive nature and poor survival rate, it ranks sixth among all cancers in mortality. Despite these facts, esophageal cancer receives very little mention when compared with other cancers such as lung, breast, and colon in terms of health promotion and education. Special note, however, should be given to the fact that esophageal cancer is one of the very few cancers that is contributing to increasing death rates (20%) among males in the United States. Understanding and delineating the epidemiology of esophageal cancer will be the key to elucidating the causes and risk factors for esophageal cancer and thus the cornerstone of developing any prevention strategies.
Epidemiology
Age
The incidence of esophageal cancer increases with age. This pattern is similar in developing and developed countries. On average, adenocarcinoma generally is acquired 10 years earlier than squamous cell carcinoma ( Table 1 ).
| Squamous Cell Carcinoma | Adenocarcinoma | |
|---|---|---|
| Age | 60–70 years; median 62.7 years | 50–60 years; median 53.4 years |
| Gender | Male | Male |
| Socioeconomic status | Low | Middle to upper |
| Locations | 75% midesophagus | 94% distal esophagus |
| Symptoms | Progressive dysphagia, odynophagia, halitosis, unintentional weight loss, chest pain | Progressive dysphagia, odynophagia, halitosis, unintentional weight loss, chest pain |
| Environmental factors | Alcohol, cigarette smoking, mate-tea ingestion, betel-nut chewing, caustic ingestion, esophageal radiation exposure, high-fat diet, low vitamin diet [vitamin C, folate, beta-carotene, vitamin E], drinking hot liquids (>70°C) | Cigarette smoking, high-fat diet, low vitamin diet [vitamin C, folate, beta-carotene, vitamin E] |
| Medical conditions | Head/neck squamous cell carcinoma,Plummer-Vinson [Patterson-Kelly] syndrome, achalasia, tylosis, celiac disease, human papilloma virus infection, Helicobacter pylori infection | Barrett’s metaplasia, Zollinger-Ellison syndrome, scleroderma, prior esophageal dilations, gastroesophageal reflux disease, obesity |
Gender
In terms of gender differences, for squamous cell carcinoma in the Western world it occurs three to four times more often in males than females, although in the esophageal cancer belt, it is approximately a one to one ratio. for adenocarcinoma, however, males are six to eight times more likely to develop this particular form of esophageal cancer than females.
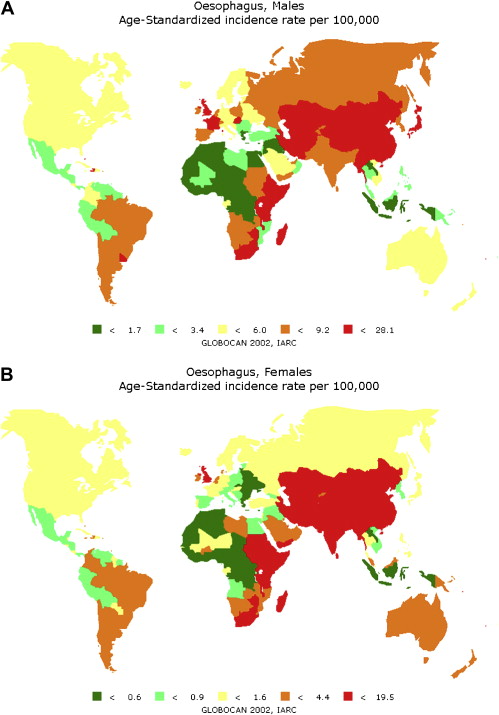
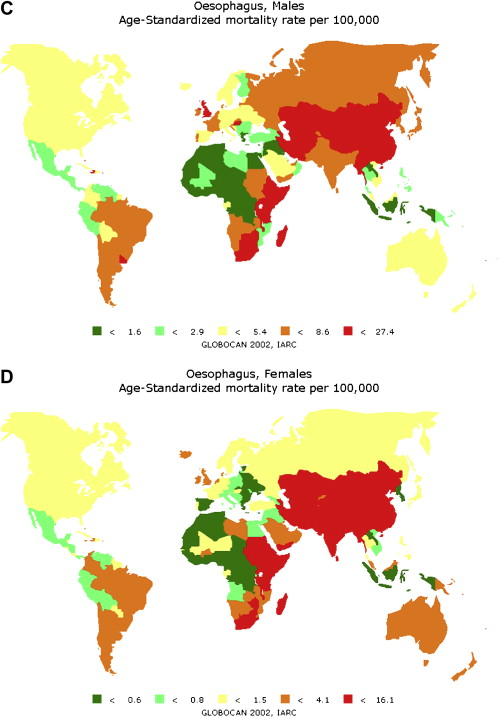
World
Esophageal cancer is an uncommon cancer. In terms of new (incident) cases of cancer, esophageal cancer is ranked as the eighth most common cancer in the world. At this point, it is important to differentiate esophageal cancer into its two histopathological subtypes (squamous cell carcinoma and adenocarcinoma), as the epidemiology between the two groups is vastly different. Surprisingly, over the last 30 years, there has been a major shift in the dominating histologic subtype of esophageal cancer in the Western world; previously, it was squamous cell carcinoma, and now it is adenocarcinoma. It is important to note that the classification of esophago–cardial adenocarcinomas also may explain the increase in this lesion. The wide geographic variation in incidence of esophageal cancer is marked, as is the mortality rates ( Fig. 1 ). The variation in incidence for esophageal cancer can differ as much as 500-fold from one part of the world to another. It is known that Asian countries, in particular China, India, Pakistan, and Japan, have the highest rates of esophageal cancer in the world; therefore countries mentioned in the following sections highlight those that have changed substantially over time or those that may not be well known as having high incidence of esophageal cancer.
United States
It is surprising to find that in the United States the incidence of esophageal cancer among both males and females ranks in the top 20 countries. Disturbingly, African American males from the District of Columbia rank number five and African American females from the state of Connecticut rank number 14 ( Tables 2 and 3 ). Moreover, African Americans from two additional states (South Carolina and Georgia) also are listed in the top 20 locations for esophageal cancer in the world. In the United States, squamous cell carcinoma remains the predominant subtype among African Americans, who have esophageal cancer rates six times higher than whites.
| Country, State/Province | Cases | Age Standard Rate |
|---|---|---|
| 1. China, Jiashan | 254 | 20.2 |
| 2. China, Zhongshan | 532 | 16.5 |
| 3. Japan, Miyagi | 1656 | 15.4 |
| 4. Zimbabwe, Harare: African | 219 | 15.1 |
| 5. USA, District of Columbia: black | 149 | 14.8 |
| 6. France, Calvados | 327 | 14.6 |
| 7. United States, South Carolina: black | 377 | 14.4 |
| 8. France, Somme | 271 | 14.1 |
| 9. Uganda, Kyadondo | 125 | 14.1 |
| 10. France, Manche | 268 | 13.1 |
| 11. Brazil, Brasilia | 262 | 13.1 |
| 12. Japan, Yamagata | 892 | 13.0 |
| 13. France, Loire-Atlantique | 503 | 12.7 |
| 14. Japan, Hiroshima | 503 | 12.1 |
| 15. Brazil, Sao Paulo | 2406 | 12.0 |
| 16. Brazil, Cuiaba | 72 | 11.7 |
| 17. United Kingdom, Scotland | 2391 | 11.7 |
| 18. United States, Georgia: Black | 470 | 11.1 |
| 19. France, Bas-Rhin | 370 | 10.9 |
| 20. United States, District of Columbia | 179 | 10.8 |
Related posts:
 Environmental Causes of Esophageal Cancer
Genetic Variations in Esophageal Cancer Risk and Prognosis
The Role of FDG-PET and Staging Laparoscopy in the Management of Patients with Cancer of the Esophagus or Gastroesophageal Junction
Environmental Causes of Esophageal Cancer
Genetic Variations in Esophageal Cancer Risk and Prognosis
The Role of FDG-PET and Staging Laparoscopy in the Management of Patients with Cancer of the Esophagus or Gastroesophageal Junction
 Traditional Chinese Medicinal Herbs in the Treatment of Patients with Esophageal Cancer: A Systematic Review
Future Developments in Esophageal Cancer Research
Screening, Surveillance, and Prevention for Esophageal Cancer
Traditional Chinese Medicinal Herbs in the Treatment of Patients with Esophageal Cancer: A Systematic Review
Future Developments in Esophageal Cancer Research
Screening, Surveillance, and Prevention for Esophageal Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


