Acute variceal bleeding (AVB) is a milestone event for patients with portal hypertension. Esophageal varices bleed because of an increase in portal pressure that causes the variceal wall to rupture. AVB in a patient with cirrhosis and portal hypertension is associated with significant morbidity and mortality. The initial management of these patients includes proper resuscitation, antibiotic prophylaxis, pharmacologic therapy with vasoconstrictors, and endoscopic therapy. Intravascular fluid management, timing of endoscopy, and endoscopic technique are key in managing these patients. This article reviews the current endoscopic hemostatic strategies for patients with AVB.
Key points
- •
Acute variceal bleeding (AVB) is a serious complication of patients with portal hypertension.
- •
Initial management includes appropriate volume replacement, transfusion of blood to keep hemoglobin levels around 7 to 8 g/dL, antibiotic prophylaxis, and endotracheal intubation in selected cases.
- •
Standard of care mandates early administration of vasoactive drug therapy followed by endoscopic band ligation (EBL) or injection endoscopic sclerotherapy (if EBL cannot be performed) within the first 12 hours of patient presentation.
- •
Patients who fail endoscopic hemostasis therapy may require the temporary placement of balloon tamponade or an esophageal stent; however, experience with esophageal stents is limited and use of balloon tamponade is associated with potentially lethal complications such as aspiration and perforation of the esophagus.
- •
Both modalities should be available for potential use and all patients surviving an episode of AVB should undergo secondary prophylaxis in order to prevent variceal rebleeding.
The development of portal hypertension in cirrhosis changes the natural course of patients with chronic liver disease because it has several consequences, including the development of gastroesophageal varices, variceal bleeding, ascites, hepatorenal syndrome, and hepatic encephalopathy. The initial appearance of varices in patients with compensated cirrhosis indicates a progression of the disease from a low-risk state to an intermediate state, but once bleeding occurs this indicates decompensation and an increased risk of death. Although mortalities caused by acute variceal bleeding (AVB) have declined from nearly 60% to 15% to 20% at 6 weeks in the past 3 to 4 decades, there is still a significant risk of recurrence and of morbidity and mortality. All patients surviving an AVB should therefore receive secondary prophylaxis. This article reviews the current management approach of patients with AVB with particular emphasis on endoscopic hemostatic techniques for bleeding varices.
Natural history and diagnosis of acute variceal bleeding
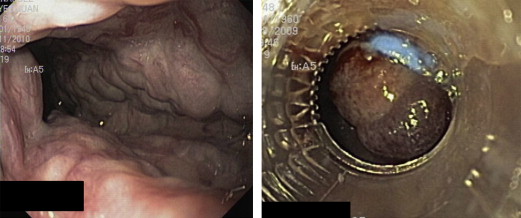
Patients with esophageal varices have an incidence of AVB that ranges from 4% to 15% per year depending on the severity of liver disease, variceal size, presence of red wale markings, and a hepatic venous pressure gradient (HVPG) value greater than 12 mm Hg. In most cases (80%), patients with cirrhosis and gastrointestinal bleeding have gastroesophageal varices as the cause of hemorrhage. Thus upper gastrointestinal bleeding in patients with cirrhosis must be presumed to be variceal in origin until proved otherwise. Although the clinical history is highly reliable in assuming the diagnosis of AVB, the gold standard for the diagnosis is upper endoscopy. Endoscopy can show active blood spurting or oozing from a varix (this can be present in 15% of patients) ( Fig. 1 ), a white nipple or clot adherent to a varix, or the presence of varices without other potential sources of bleeding in the upper gastrointestinal tract. Although acute bleeding from varices may cease spontaneously in nearly half of patients, rebleeding rates are significantly high (30%–40%) if patients are not treated appropriately. The highest risk occurs within the 48 hours following the index bleed and most of the rebleeding episodes occur with the first 14 days. Initial endoscopic failure to control bleeding occurs most commonly in patients with Child class C cirrhosis, concomitant bacterial infection, portal vein thrombosis, active spurting of a varix, and an HVPG greater than 20 mm Hg.
Survival from an episode of AVB has improved greatly: from 42% in the 1980s to the current rates of 80% to 85%. This improvement has been caused by overall improvements in intensive care, volume repletion, pharmacologic and endoscopic therapy, implementation of transjugular intrahepatic portosystemic shunts (TIPS), and prophylaxis for bacterial infections. Current estimates of mortality from uncontrolled bleeding are 4% to 8%. Approximately one-third of the deaths are a direct consequence of bleeding and the remainder are caused by liver failure, infections, and renal failure.
Recent studies stress the importance of identifying good prognostic markers in patients with episodes of acute bleeding. Although it is well known that HVPG greater than 20 mm Hg is associated with a high risk of 5-day treatment failure to control bleeding, obtaining this measurement is invasive and not available in all centers. However, easily obtainable clinical variables (Child-Pugh class C, systolic blood pressure <100 mm Hg at admission, and nonalcoholic causes of cirrhosis) are also associated with 5-day treatment failure to control bleeding, which means that the presence of any of these variables on admission helps clinicians to plan aggressive management and further therapies that may be needed if there is no good response to initial standard-of-care treatment.
Natural history and diagnosis of acute variceal bleeding
Patients with esophageal varices have an incidence of AVB that ranges from 4% to 15% per year depending on the severity of liver disease, variceal size, presence of red wale markings, and a hepatic venous pressure gradient (HVPG) value greater than 12 mm Hg. In most cases (80%), patients with cirrhosis and gastrointestinal bleeding have gastroesophageal varices as the cause of hemorrhage. Thus upper gastrointestinal bleeding in patients with cirrhosis must be presumed to be variceal in origin until proved otherwise. Although the clinical history is highly reliable in assuming the diagnosis of AVB, the gold standard for the diagnosis is upper endoscopy. Endoscopy can show active blood spurting or oozing from a varix (this can be present in 15% of patients) ( Fig. 1 ), a white nipple or clot adherent to a varix, or the presence of varices without other potential sources of bleeding in the upper gastrointestinal tract. Although acute bleeding from varices may cease spontaneously in nearly half of patients, rebleeding rates are significantly high (30%–40%) if patients are not treated appropriately. The highest risk occurs within the 48 hours following the index bleed and most of the rebleeding episodes occur with the first 14 days. Initial endoscopic failure to control bleeding occurs most commonly in patients with Child class C cirrhosis, concomitant bacterial infection, portal vein thrombosis, active spurting of a varix, and an HVPG greater than 20 mm Hg.
Survival from an episode of AVB has improved greatly: from 42% in the 1980s to the current rates of 80% to 85%. This improvement has been caused by overall improvements in intensive care, volume repletion, pharmacologic and endoscopic therapy, implementation of transjugular intrahepatic portosystemic shunts (TIPS), and prophylaxis for bacterial infections. Current estimates of mortality from uncontrolled bleeding are 4% to 8%. Approximately one-third of the deaths are a direct consequence of bleeding and the remainder are caused by liver failure, infections, and renal failure.
Recent studies stress the importance of identifying good prognostic markers in patients with episodes of acute bleeding. Although it is well known that HVPG greater than 20 mm Hg is associated with a high risk of 5-day treatment failure to control bleeding, obtaining this measurement is invasive and not available in all centers. However, easily obtainable clinical variables (Child-Pugh class C, systolic blood pressure <100 mm Hg at admission, and nonalcoholic causes of cirrhosis) are also associated with 5-day treatment failure to control bleeding, which means that the presence of any of these variables on admission helps clinicians to plan aggressive management and further therapies that may be needed if there is no good response to initial standard-of-care treatment.
Initial management
The most important initial step in providing adequate care for patients with AVB consists of (1) providing optimal hemodynamic management with cautious correction of hypovolemia, (2) preventing complications, and (3) stopping the hemorrhage. An established protocol that takes into account adequate volume resuscitation, airway management, prophylactic antibiotics, administration of vasoconstrictors, and therapeutic endoscopy should be followed in all cases of AVB.
A decision to secure the airway before endoscopy should be considered in patients with hepatic encephalopathy and those actively vomiting blood because of the high risk of pulmonary aspiration. Although there are scarce data on this practice and some investigators claim intubation is not safe, others have shown benefits in improving patient outcome. Volume resuscitation with plasma expanders should be instituted in order to keep systolic blood pressure at 100 mm Hg. This measure ensures adequate tissue perfusion with avoidance of hemodynamic shock; hemodynamic shock can cause renal failure, which is associated with an increased risk of death. In contrast, overtransfusion should be avoided because it may induce rebound increases in portal pressure and variceal rebleeding. Blood transfusions should aim for a hemoglobin (Hb) level of 7 g/dL, except in patients with active ongoing bleeding or with ischemic heart disease. A recent study that compared a restrictive transfusion policy that administered blood products if Hb levels decreased to less than 7 g/dL with a liberal policy (transfusion if Hb <9 g/dL) showed that the probability of survival was significantly higher in patients with cirrhosis and Child-Pugh class A or B disease who were assigned to the restrictive policy group. Moreover, within the first 5 days, the portal-pressure gradient increased significantly in patients in the liberal strategy group but not in patients assigned to the restrictive strategy group.
There are no evidence-based data to support the routine use of platelet transfusion or fresh frozen plasma administration. Current consensus and expert opinion suggest that, in patients with platelet counts less than 50,000 per μL and/or with an International Normalized Ratio greater than 1.5, it is prudent, weighing the risks and benefits, to consider transfusion of platelets and/or fresh frozen plasma before the procedure. Bacterial infections are a poor prognostic indicator in AVB. The most common infections are spontaneous bacterial peritonitis, urinary tract infections, and pneumonia. Prophylactic antibiotics in patients with AVB reduce the risk of rebleeding and mortality, thus all patients on admission should receive them. Norfloxacin 400 mg by mouth twice daily for 7 days may be given; however, patients with hypovolemic shock, ascites, malnutrition, encephalopathy, or bilirubin greater than 3 mg/dL should receive intravenous ceftriaxone (1 g/d) because it is more effective than oral norfloxacin in the prophylaxis of bacterial infections in patients with cirrhosis and AVB.
Prompt initiation of vasoactive drugs and timing of endoscopy should be planned from the time the patient arrives at the hospital. This promptness facilitates establishing a diagnosis and performing therapy. Emergency endoscopy should be performed within the first 12 hours after admission. If patients are actively vomiting blood, it should be performed once the patient has been hemodynamically stabilized in a monitored unit. Recent data indicate that the early placement of TIPS (within 72 hours) for patients with AVB with Child B actively bleeding or Child C cirrhosis (<13 points) is associated with a significant reduction in rebleeding and mortality and thus should be considered in such cases.
Specific treatment
Vasoconstrictors
In suspected variceal bleeding, vasoactive drugs (which reduce portal pressure and decrease variceal blood flow) need to be given as soon as possible and before upper endoscopy. This advice is supported by randomized controlled trials (RCTs) and meta-analyses showing that the use of vasoactive drugs achieves hemostasis and reduces the rate of active bleeding, making endoscopy easier to perform for diagnostic and therapeutic purposes. In addition, these drugs reduce rebleeding and all-cause mortality among patients with cirrhosis and AVB. Two types of drugs are used: vasopressin and its analogues (terlipressin) and somatostatin and its analogues (octreotide/vapreotide) ( Table 1 ).
| Drug | Dose |
|---|---|
| Terlipressin | IV bolus 2 mg every 4 h for 24–48 h then 1 mg every 4 h |
| Somatostatin | IV bolus 250 μg followed by infusion of 250–500 μg/h |
| Octreotide | IV bolus of 50–100 μg followed by infusion of 50 μg/h |
| Vapreotide | IV bolus of 50 μg followed by infusion of 50 μg/h |
Endoscopy
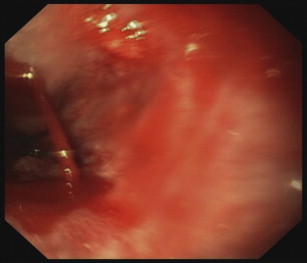
Endoscopy is one of the cornerstones of AVB management because it confirms the diagnosis and allows therapy during the same session. Endoscopic therapies for varices are designed to reduce variceal wall tension by obliteration of the varix. The 2 endoscopic methods available for AVB are endoscopic sclerotherapy (EST) and endoscopic band ligation (EBL) ( Fig. 2 ). Endoscopic therapy should be used in conjunction with vasoconstrictors. This strategy is strongly supported by several trials and guidelines showing that the efficacy of both emergency EST and EBL is significantly improved when they are associated with pharmacologic treatment.
Endoscopic sclerotherapy
For AVB, this technique consists of the injection of a sclerosing agent into the variceal lumen (intravariceal injection); this causes thrombosis of the varix and inflammation of the surrounding mucosa that with time creates a scar over the esophageal wall. EST is performed with an injection catheter (needle tip, 23 or 25 gauge) and the sclerosant solution. The most common sclerosants are ethanolamine oleate (5%), polidocanol (1%–2%), or sodium morrhuate (5%). The first injection of 1 to 2 mL of the sclerosant should be placed immediately below (distal to) the bleeding site. Afterward, the remaining varices are injected with 1 to 2 mL adjacent to the bleeding varix. The main objective is to target the lower esophagus near the gastroesophageal (GE) junction. In most cases, up to 15 mL of a sclerosant solution are required. The advantages of using EST for AVB are mainly related to the technique being user friendly because the injection catheter fits through the working channel of a diagnostic gastroscope and does not require a second oral intubation. In addition, there is rapid formation of a thrombus. Drawbacks include a variety of local and systemic side effects, including substernal chest pain, fever, dysphagia, and pleural effusion. Esophageal ulcers are common and in 20% of patients they may cause bleeding. Bacteremia may occur in up to 35% of patients and lead to other complications such as spontaneous bacterial peritonitis or distal abscesses. Other complications include esophageal strictures, perforations, mediastinitis, pericarditis, chylothorax, esophageal motility disorders, and acute respiratory distress syndrome.
Endoscopic band ligation
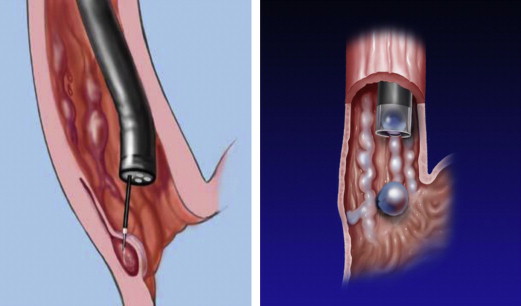
This technique consists of placing elastic bands on the varices in order to occlude the varix and cause thrombosis and the subsequent necrosis of the mucosa. The bands fall off in 5 to 8 days leaving a superficial mucosal ulceration that heals and eventually scars. Clinical trials and a meta-analysis have shown that EBL is better than EST for all major outcomes, including initial control of bleeding (primary hemostasis), recurrent bleeding, side effects, time to variceal obliteration, and survival.
There are several multiband devices available for EBL; the most common are the Saeed Multiple Ligator (Wilson-Cook Medical, Inc) and the Speedband (Boston Scientific Corporation). They have between 4 and 10 preloaded bands, but in most cases the ligators with 6 or 7 bands are used. All work on the same principle, which is placement of elastic bands on the varix after it is sucked into a clear plastic cylinder attached to the tip of the endoscope. After the diagnostic endoscopy is performed and the variceal bleeding site is identified, the endoscope is withdrawn and the ligation device is loaded. After reintubation with the ligation device placed on the endoscope, the varix (usually in the distal third of the esophagus) is identified and the tip is pointed toward it and continuous suction applied so that it fills the cap. Once inside the cap has a red-out sign, the band can be deployed ( Fig. 3 ). After the varix is ligated, the endoscope should not be advanced, to avoid dislodgement of the bands, which is why banding should always commence in the most distal portion of the esophagus near the GE junction. Bands are applied in a spiral pattern progressing the esophagus up (proximally) until all major columns of varices of the lower third of the esophagus (usually no more than 10 cm above the GE junction) are banded. If there is active bleeding and there is a limited view, the bands should be placed at the GE junction. This method reduces ongoing bleeding and further bands can be fired afterward until active bleeding ceases.