Fig. 13.1
Trocar placement
Reduction of the Hernia Contents
In open surgery, it is important not to try to reduce the hernia contents during induction of anesthesia, since it is possible to introduce a viable ischemic bowel into the intra-abdominal compartment, with the risk of perforation during the immediate postoperative period. It is important to keep the hernia contents in the bag until opened and subsequent assessment of viability is made.
If the bowel is reduced spontaneously, its location through the hernia ring is difficult and ineffective. For identification, it is feasible to use the laparoscope introduced through the hernia ring and then to evaluate whether or not bowel viability exists. This technique is called hernioscopy [3].
Hernioscopy is laparoscopy traversing a hernia sac used in the course of traditional treatment for groin hernia, and it may be both diagnostic and therapeutic. See Fig. 13.2.
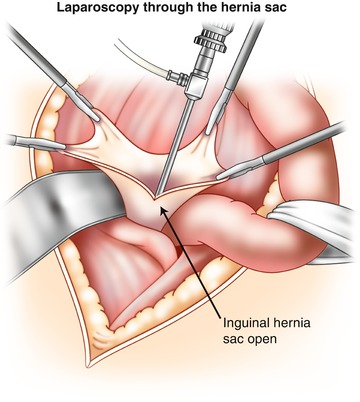
Fig. 13.2
Hernioscopy
In laparoscopic surgery, we are able to assess the vitality of the bowel even before the induction of anesthesia, because we can view it directly. The establishment of pneumoperitoneum facilitates spontaneous reduction.
In the case of nonreduction, there are several techniques for reintroducing the abdomen [4] (Fig. 13.3):
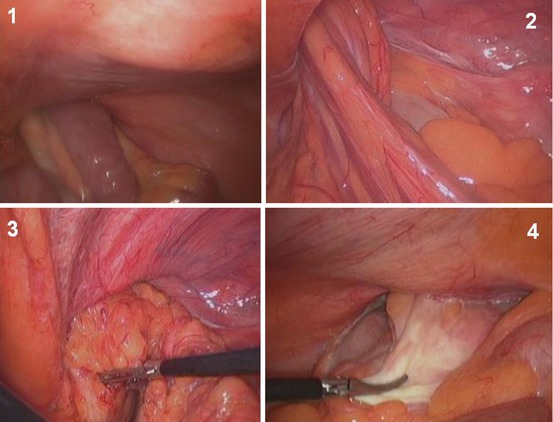
Fig. 13.3
TAPP in inguinal hernia, incarcerated. 1 Small bowel incarcerated in right inguinal hernia. 2 Reduction of the hernia with traction control. 3 Incarcerated epiplon in right inguinal hernia. 4 Colon incarcerated in left inguinal hernia
Traction control, avoiding handling it directly. First try to reduce omentum and get more space so as to facilitate the reduction of the bowel loop.
Opening the hernial orifice in its medial part, avoiding damage to epigastric vessels. This maneuver sections ring constriction and facilitates the complete reduction of the content.
Treatment of Content
Once the hernia content is reduced, the bowel integrity is evaluated based on its coloration and peristalsis. If it is necessary to do loop resection when you are doing an open inguinal access, you may do so through the inguinal or by midline laparotomy depending on the difficulty.
During the laparoscopic approach, intestinal resection can be performed laparoscopically or by minilaparotomy assistance, which later will be used to extract the surgical specimen. This surgical approach decreases pain and postoperative recovery time for patients when compared with conventional open surgery [5].
Treatment of Hernia Defect
Until recently, all surgeries that required a bowel resection contraindicated the use of mesh because of the probability of infection by this prosthetic. However, according to scientific evidence, there is currently no reason not to use mesh for the treatment of urgent hernia defect surgery in the abdominal wall. Wisocky et al. objectified only two prosthetic infections in 56 patients treated for emergency inguinal hernias by the Lichtenstein technique [6].
Related posts:
 Prostheses in Laparoscopic Inguinal Hernia Repair
Prostheses in Laparoscopic Inguinal Hernia Repair
 Basic Concepts in Laparoscopic Hernia Repair
Basic Concepts in Laparoscopic Hernia Repair
 Laparoscopic Ventral Hernia Repair
Laparoscopic Ventral Hernia Repair
 Prostheses Fixation During Laparoscopic Inguinal Hernia Repair
Prostheses Fixation During Laparoscopic Inguinal Hernia Repair
 Current Advances and New Frontiers in Laparoscopic Hernia Repair
Current Advances and New Frontiers in Laparoscopic Hernia Repair
 Laparoscopic Approach in Other Hernias: Subcostal, Xiphoid, Lumbar, Suprapubic, Parastomal, and Spigelian
Laparoscopic Approach in Other Hernias: Subcostal, Xiphoid, Lumbar, Suprapubic, Parastomal, and Spigelian
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


