Fig. 11.1
Patient ready for ECIRS in the Galdakao-modified supine Valdivia position

Fig. 11.2
Adequate padding of the legs’ stirrups to prevent pressure damages
Check according to your internal hospital procedures the identity of the patient, the kind of procedure, and the side to be operated (that has to be correctly marked).
Check that the operating table is radiolucent, can be sufficiently translated leaving the abdomen free of radiopaque obstacles and easily host the C-arm of the fluoroscopy for radiological control during the procedure in the areas of interest, and can be arranged with the leg stirrups for lithotomic position.
If the OR is too narrow, incline the operating table, leaving more space on that side to be operated; the floor may be prepared with absorbing materials, in order to avoid inadvertent spilling of irrigation fluids all around.
The first landmark is the posterior axillary line (Fig. 11.3) that has to be drawn with an undeletable pen possibly with the patient standing, arm up, or in any case with the patient pure supine before starting the positioning maneuvers.

Fig. 11.3
The posterior axillary line is drawn in the simple supine position
The patient is then positioned supine on the operating table, near to the border of the side with the stone to be operated (this is important to increase free mobility of the nephroscope), then prepared and anaesthetized.
The arm contralateral to the side to be operated lies abducted of less than 90° and slightly flexed on a padded support, or along the body, for anesthesiological management (Fig. 11.4).

Fig. 11.4
Arrangement of the contralateral arm for venous access
The ipsilateral arm of the patient crosses the chest lying on it or supported, further elevating the posterior axillary line (Fig. 11.5). It is preferable not to use metallic arm support, because this interferes with the X-ray beam, should the C-arm be tilted cephalad, during fluoroscopic-controlled access creation. A padded support maintains the arm with an angle less than 90° with that of the operating table.

Fig. 11.5
Arrangement of the ipsilateral arm, adequately fixed (a) and with a cushion under it to prevent peripheral nerve damage (b)
The lumbar region is lifted approximately 20° and exposed. There are several ways to tilt the patient. Valdivia Urìa in his original description used an emptied 3 l saline irrigation bag for transurethral resection, inflating it with air and closing the outflow tube with a Kocher forceps, allowing volume control until the best position is found (Fig. 11.6a, courtesy of Dr. Gaspar Ibarluzea). Others use two silicone gel pads or two “plum cake”-shaped jelly pillows, one under the shoulder and another under the gluteal region, leaving the lumbar region free and creating a space preventing instruments collision (Fig. 11.6b). There is also an inflatable device called “Pelvic-Tilt” (OR comfort LLC, Glen Ridge, NJ, USA) (Fig. 11.6c). This device has a non-inflated flap extending from one side. The flap is placed under the lumbar region opposite to the stone, while the inflatable portion is placed under the stone side. The weight of the patient on the flap prevents the lateral shifting of the pillow.
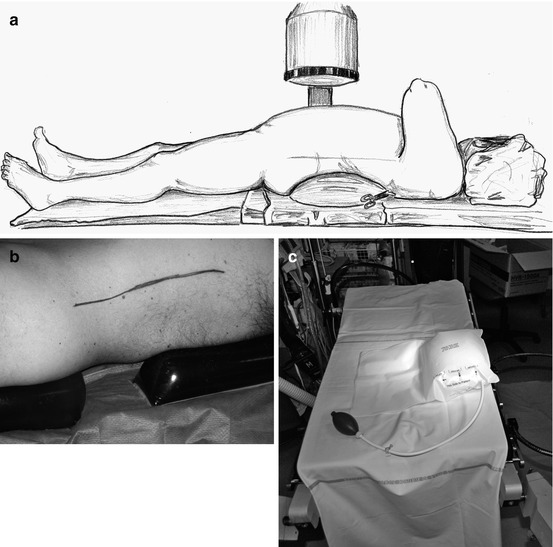
Fig. 11.6
Methods for elevating the flank to be operated: (a) saline bag under the flank, original method (The drawing is a courtesy of Dr. Gaspar Ibarluzea), (b) jelly pillows under the gluteus and the thorax, (c) inflatable device under the flank
The further landmarks can now be drawn: the lower margin of the 12th rib and the upper margin of the iliac crest (Fig. 11.7).

Fig. 11.7
When the patient is in the right position, the remaining reference lines are drawn (12th rib and iliac crest)
Then the patient is put in a modified lithotomy position, very similar to that used during a semirigid retrograde ureteroscopy, with both glutei on the inferior border of the operating table. The ipsilateral leg is slightly abducted and extended, and the contralateral leg is lifted and partially flexed (Fig. 11.8). Both leg stirrups should be adequately padded, possibly with gelatins as well.
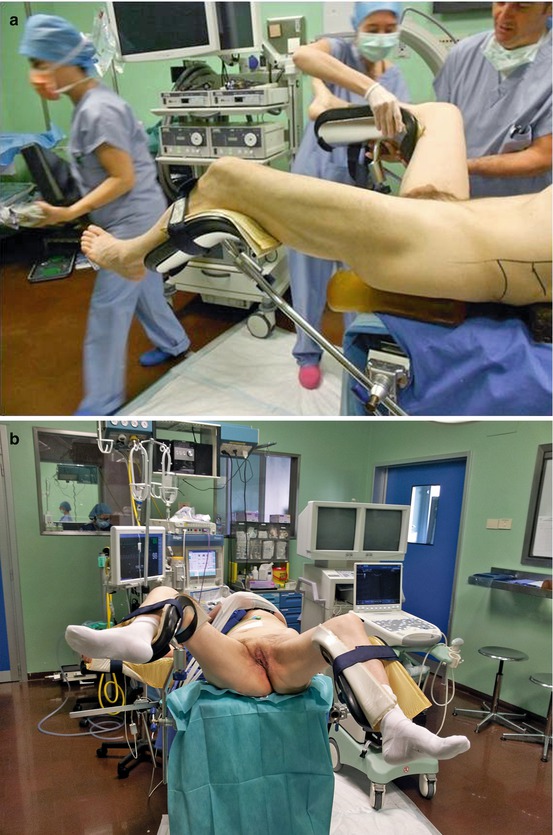
Fig. 11.8
Arrangement of the legs: the ipsilateral one is slightly extended and the contralateral one well abducted. Lateral (a) and frontal (b) views
After positioning maneuvers, check again for possible corrections (especially of the upper and lower limbs) and fix everything with the aid of Peha-haft or similar.
11.2 Sterile Draping of the Patient and Preparation of the Surgical Field
Disinfection of the skin comprises the lumbar region, the anterior abdominal wall, the external genitalia, and the perineum (Fig. 11.9) (see also Chap. 19).

Fig. 11.9
Final sterile draping with the bags for retrieving irrigation fluids
The sterile draping does not require to be changed intraoperatively. We use a standard cystoscopy set which is not entirely unfolded towards the abdomen and chest, and then the lumbar region is draped with standard abdominal adhesive drapes or with a modified cystoscopy set.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








