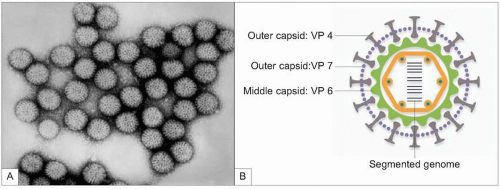
 3.1 A: Electron microscopy of rotavirus particles from an infant with acute diarrhoea (courtesy Centers for Disease Prevention and Control, Atlanta, GA, USA); B: schematic of the complete rotavirus particle with structural proteins in the different shells. |
excretion of viral particles in the days prior to clinical symptoms and continuing through to its resolution. Rotavirus is a seasonal infection and in temperate climates infections peak during the winter months3. In bacterial enteric infection transmission can be through contaminated water or foodstuffs.
Table 3.1 Main agents of infectious acute diarrhoea | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 3.2 Pathogenesis of viral diarrhoea: rotavirus infects selectively mature enterocytes on the tips of small intestine villi, leading to their destruction and villi atrophy. (Courtesy Faculty of Biological Sciences, University of Barcelona, Barcelona, Spain.) |
Table 3.2 Main features of viral agents | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 3.3 Clinical features suggestive of bacterial diarrhoea | |
|---|---|
|
|
include stool cultures for bacteria and detection of faecal viral antigen by enzyme immunoassay (EIA), agglutination with latex particles, or immunochromatography.
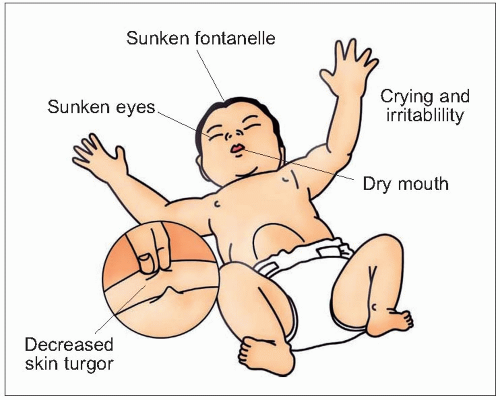 3.3 Signs of dehydration. |
|
Table 3.6 Recommendations for faecal laboratory study | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
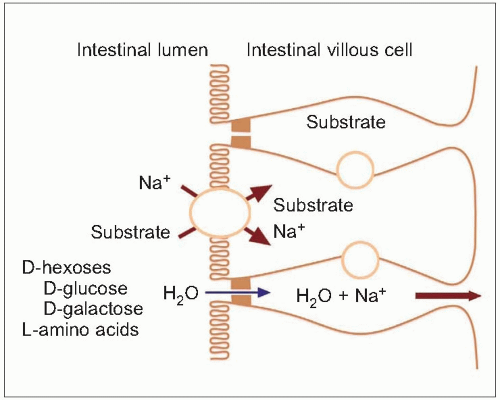 3.4 Diagram to show the processes involved in cotransport of organic solutes and sodium and secondary water absorption. |
Table 3.7 Oral rehydration solution composition | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


