Table 1-1 Recipe to Improve Biopsy Quality and Interpretation Dramatically | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
biopsy specimens. These are areas, which normally lack folds or valves, especially the esophagus, gastric antrum, and duodenal bulb. In these areas, the endoscopist should partially collapse the lumen by suctioning out insufflated air just prior to biopsy. In the esophagus, the tip of the endoscope may be deflected 90 degrees against the wall, thus allowing the forceps to be advanced en face from close up (“turn-and-suction” biopsy technique). The esophageal mucosa is still the most difficult area in the gastrointestinal tract from which to obtain sufficiently deep, high-quality biopsy specimens.
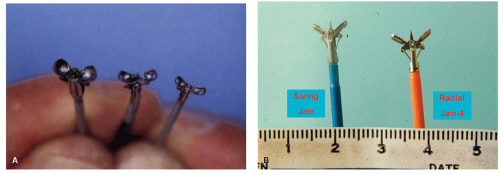 Figure 1-1. A: Endoscopic pinch biopsy forceps. These are passed through a side channel in the endoscope. The forceps on the right is small and fits into a 1.8-mm pediatric-sized scope but commonly yields suboptimal biopsy specimens. The middle forceps is often the standard size fitting into a 2.8-mm endoscopy channel. The forceps on the left has an 8-mm open span and is the best; it requires a larger biopsy channel and hence a slightly larger-diameter endoscope. Most of these forceps have a central spike to help impale the mucosa. B: Biopsy forceps that produce larger biopsies. The swing jaw mechanism enables easier cup positioning for biopsy sites approached tangentially such as in the esophagus. That on the right produces jumbo biopsy-sized pieces of tissue but fits down a scope’s standard 2.8-mm biopsy channel. |
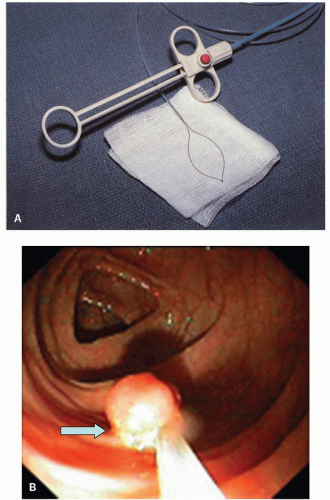 Figure 1-2. Electrocautery snare used for polypectomy. A: The device is attached to an electrocautery unit. The handle is used to extend and retract the snare. B: Snare tightened around the stalk of a polyp in transverse colon. Some stalks can be intentionally left behind (arrow) to avoid cauterizing too close to the wall (possibly making a mockery of proximity to the cauterized margin as an indication of nodal metastases if this can be deliberately varied). |
If the distal aspect (closest to the endoscope, and the most tempting) is injected first, the polyp can be tilted away from the colonoscope, making subsequent resection more difficult. If a bleb does not immediately form, the needle can be slowly withdrawn and lifted slightly while injecting until bleb formation is observed. It is often helpful to inject at the lateral margin of the cushion produced by the previous injection (which has already separated the mucosal layer from the muscularis propria). However, if a bleb does not form, the needle may have penetrated the colon wall and so the fluid is being injected into the peritoneum. Alternatively, the failure to lift may indicate the presence of invasive cancer that is tethering the polyp to the underlying muscularis propria. This is called the “nonlifting sign.”3
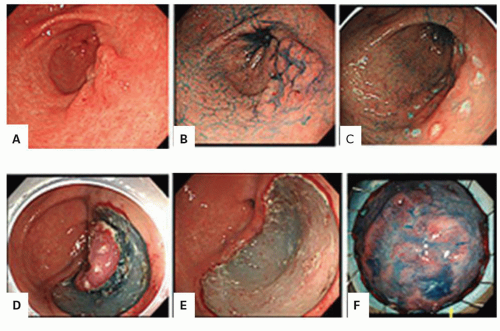 Figure 1-3. Endoscopic submucosal dissection. A: Large bowel lesion to be resected. B: The lesion is highlighted using chromoscopy. C: The limitation of the dissection is outlined by tattooing. D: The lesion has almost been removed. E: Removal is complete leaving a smooth base (F) pathology specimen. (Courtesy: Dr. C. Streutker.) |
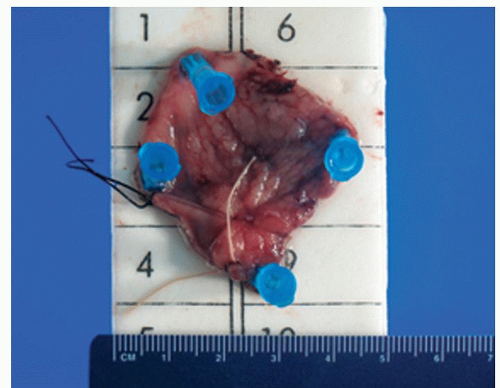 Figure 1-4. Pinned out specimen from rectum obtained by transanal excision. |
the endoscope and the suction line (Fig. 1-6). If the duodenum is “dry,” a segment of mucosa can be rubbed with the cytology brush and smears prepared for parasite examination. It can be useful to obtain aspirated material or brush smears from the duodenum whenever small-bowel biopsies are being done in the evaluation of patients with diarrhea.
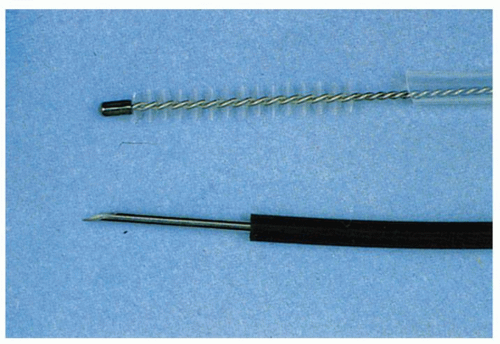 Figure 1-5. Accessories used to complement endoscopic biopsy. Top: Cytology brush. This is passed through the biopsy channel enclosed in a plastic sheath and is then advanced, using a handle at the head end. Bottom: A 21-gauge needle or thinner is used for fine-needle aspiration, usually under ultrasound guidance for submucosal or deeper lesions. |
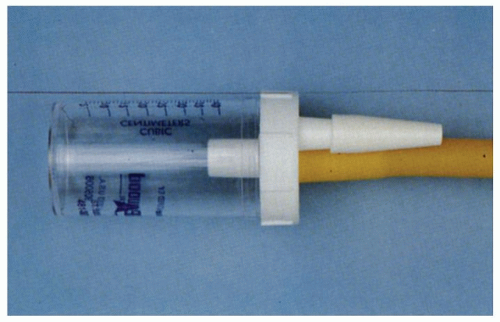 Figure 1-6. A suction trap is attached to the suction line of the endoscope to obtain luminal fluids, especially from the duodenum. |
 Figure 1-7. Balloon surrounded by mesh for esophageal cytology. This is used to screen for esophageal cancer, especially in certain high-prevalence provinces in China. The device is passed perorally into the stomach; the balloon is inflated and then removed while inflated. Thus, the surface cells are trapped in the mesh. |
and the colon. Missing some foci of inflammation in an otherwise obviously inflamed organ has much less clinical implication than missing neoplastic foci in either an inflamed or a noninflamed organ. Indigo carmine as chromogen enhances the mucosal surface by pooling in the grooves between the mucosal villi enabling the visualization of the pattern formed by the mucosal folds and pits. Acetic acid achieves the same goal by means of reversible desaturation of superficial mucosal proteins. The bottom line is that these dyes or acetic acid can accentuate mucosal pit patterns so that neoplastic ones become more evident.
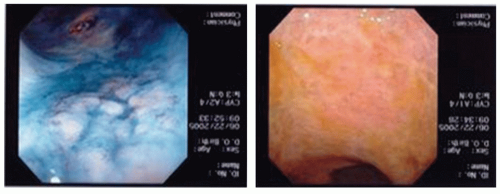 Figure 1-8. Chromoscopy in UC. The lesion on the left has been highlighted using methylene blue. In the prechromoscopy image (right), it is barely visible. |
blue dye spray with targeted biopsies was inferior to random nontargeted biopsies. Further, a higher percentage of biopsies in the random biopsy group were dysplastic (36%) compared to that of the methylene blue targeted group (26%, p = 0.05).17 A meta-analysis of nine studies comparing methylene blue chromoendoscopy with routine white light endoscopy plus biopsy revealed no incremental benefit of methylene blue chromoendoscopy over white light endoscopy.18
are endoscopically normal may actually have subtle vascular changes and NBI may identify this). It may not be as effective at identifying mass lesions as dye-based chromoendoscopy, although this requires further study. In one study, 50 patients with UC were endoscopically inspected with a scope that had the capacity for usual white light endoscopy, NBI, as well as autofluorescence—AFI (trimodal endoscopy).26 NBI can help determine the extent of inflammation and hence target where increased biopsy sampling should be undertaken. It is not clear that NBI is as good as dye spraying for colitis-associated neoplasia.
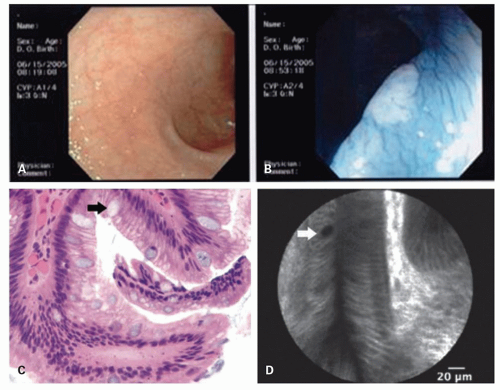 Figure 1-9. Chromoscopy in UC demonstrating how neoplastic lesions may be virtually invisible using white light (A) but highlighted using methylene blue (B). C: Histopathologic image demonstrating Barrett esophagus with no dysplasia. The surface, columnar epithelial cells are aligned in a neat row with small, basally oriented nuclei. The black arrow points out a goblet cell—the rounded bluish cell—that is the diagnostic feature of intestinal metaplasia of Barrett esophagus. D: Confocal laser endomicroscopy image of the corresponding tissue in vivo. The whiter areas are the lamina propria where fluorescein is in the highest concentration. Orderly, columnar epithelial cells line in the lamina propria as seen in the histopathologic image. The white arrow indicates a goblet cell. |
Related posts:
 Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
 Esophagus: Normal Structures, Developmental Abnormalities, and Miscellaneous Disorders
Esophagus: Normal Structures, Developmental Abnormalities, and Miscellaneous Disorders
 Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
 Small Bowel Mucosal Disease
Small Bowel Mucosal Disease
 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
 Small and Large Bowel Polyps and Tumors
Small and Large Bowel Polyps and Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


