CT Urography of the Bladder
Richard H. Cohan MD
Elaine M. Caoili MD
Jonathon M. Willatt MD
Case 10-1
History: 62-year-old male with gross hematuria.
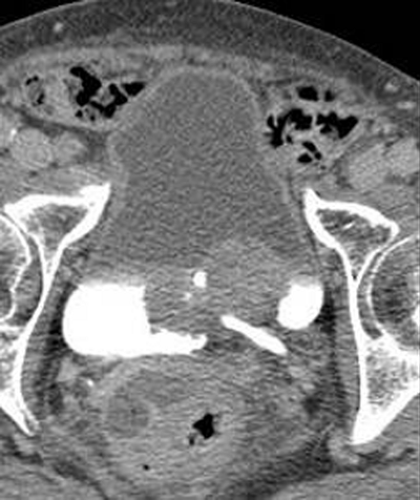 Figure 10.1 A |
 Figure 10.1 B |
 Figure 10.1 C |
Findings: An excretory phase axial CT image (A) demonstrates a small amount of excreted contrast material in the bladder. The contrast material layers dependently on the right side of the bladder. A small projection of contrast material extends medially across the midline. There is a bilobed 2.5 × 4.5-cm mass along the left posterior aspect of the bladder, which surrounds the region of the left ureterovesical junction; however, the distal left ureter is not distended. The interface between the bladder and the perivesical fat is fairly smooth throughout. The maximum and average intensity projection coronal images (B, C) also demonstrate the bladder mass.
Diagnosis: Large polypoid transitional cell carcinoma
Discussion: Large urothelial neoplasms may be detected on axial CT urography images in both opacified and unopacified portions of the bladder. These masses are often, but not always, seen on three-dimensional reconstructed images. In this case, urothelial neoplasm is the most likely diagnosis, given the rounded and lobulated appearance. Occasionally, blood clot can have this morphology.
Transitional cell carcinomas are the most common bladder malignancies, accounting for 95% of bladder cancers in areas in which schistosomiasis is not endemic (in which case squamous cell carcinoma is more common). They can have flat or polypoid/papillary morphology, with the former being more difficult to detect and also more likely to be invasive. When bladder cancers are superficial, they are often treated locally. Invasive tumors are typically treated with more aggressive surgery (e.g., cystectomy and pelvic lymph node dissection). Patients with locally treated tumors should be followed closely because recurrences and/or metachronous lesions frequently develop. Although such follow-up was previously performed primarily by obtaining periodic urine cytology specimens and cystoscopy, CT urography may also play a role in monitoring these patients.
Bladder cancer staging is performed with the TNM classification system and involves assessment of the degree of muscle invasion (with superficial being T2a and deep being T2b) and involvement of the perivesical fat (T3) or adjacent pelvic organs or pelvic sidewall (T4).
Case 10-2
History: 53-year-old male with gross hematuria.
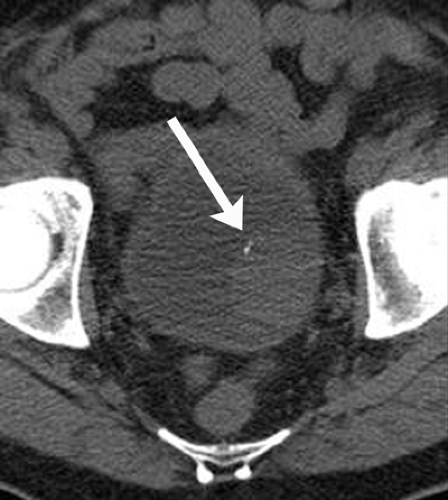 Figure 10.2 A |
 Figure 10.2 B |
 Figure 10.2 C |
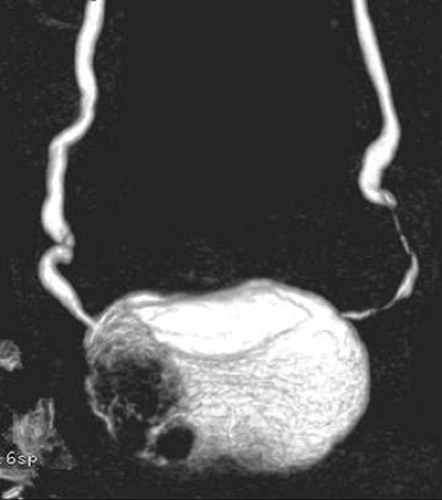 Figure 10.2 D |
Findings: Unenhanced (A), nephrographic phase (B), and excretory phase (C) axial images from a CT urogram demonstrate a large 3-cm ovoid mass in the left posterolateral aspect of the bladder. The mass is visualized on images obtained during all three phases, whether outlined by unenhanced or contrast material-containing urine in the adjacent bladder lumen. There are subtle punctate calcifications (arrow) on the surface of the mass. The mass demonstrates enhancement similar to that of the bladder wall on the nephrographic phase images. A posteroanterior volume-rendered image (D) also demonstrates the mass.
Diagnosis: Transitional cell carcinoma
Discussion: The most likely diagnosis is urothelial neoplasm, with transitional cell carcinoma (TCC) being most common. Although the differential diagnosis of a large filling defect also includes blood clot and fungus ball, these diagnoses are unlikely given the presence of the tiny surface calcifications. Rarely, inflammatory processes can have focal masslike appearances. Cystoscopy is required for definitive diagnosis. This case provides an excellent illustration of how large urothelial carcinomas that have masslike configurations may be detected by CT urography even on the unenhanced images because they are well-outlined by water attenuation urine.
Case 10-3
History: 61-year-old male with microscopic hematuria status post right nephrectomy for transitional cell carcinoma.
 Figure 10.3 A |
 Figure 10.3 B |
Findings: An excretory phase axial CT urography image (A) demonstrates extensive thickening of the right lateral and posterior wall of the bladder. Excretion of urine containing contrast material into the bladder is delayed. A thick-slab average intensity projection image (B), obtained through the anterior aspect of the bladder, also demonstrates bladder wall thickening. On this image, the thickening extends along the inferior aspect of the bladder. In addition, there is left pelvocaliectasis and an unopacified left ureter. These findings suggest that the left renal collecting system is obstructed.
Diagnosis: Transitional cell carcinoma
Discussion: In most instances, focal bladder wall thickening, as seen in this case, is due to a bladder neoplasm. Although CT cannot be used to determine depth of tumor invasion definitively, most bladder neoplasms producing this degree of wall thickening have invaded the muscular layer and are at least stage T2. Obstruction of the left renal collecting system may be due to the bladder neoplasm, which crosses the midline posteriorly to affect the left side of the bladder as well.
Cystitis can also produce bladder wall thickening but is usually diffuse. Once asymmetric bladder wall thickening is detected on CT urography, follow-up cystoscopy is warranted to allow for a definitive diagnosis.
Case 10-4
History: 57-year-old female with positive urine cytology status post nephrectomy for transitional cell carcinoma and treatment of superficial bladder cancer.
 Figure 10.4 A |
 Figure 10.4 B |
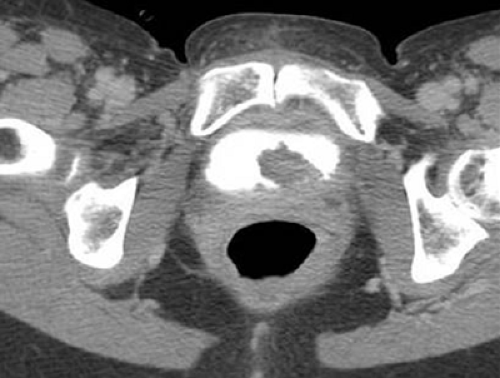 Figure 10.4 C |
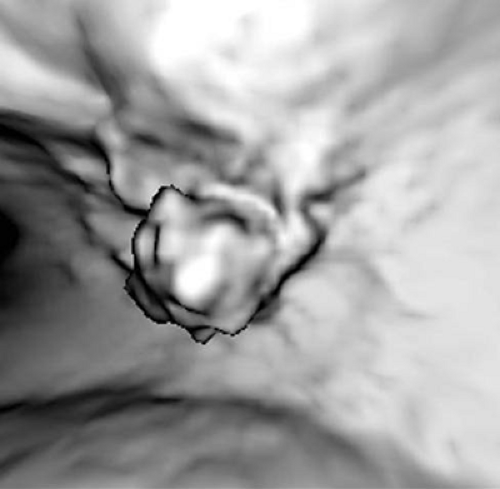 Figure 10.4 D |
 Figure 10.4 E |
 Figure 10.4 F |
Findings: Three axial excretory phase CT urographic images are provided. The first (A) demonstrates asymmetric thickening of the right anterolateral bladder wall. In addition, a small mass projects medially into the anterior aspect of the opacified portion of the bladder lumen. The second axial image (B) demonstrates a small round mass projecting into the bladder lumen from the anterior wall of the bladder. This mass is seen even though it is surrounded by unopacified urine. The third axial image (C) demonstrates a lobulated mass located inferiorly at the bladder base. Two virtual cystoscopic images (D, E) demonstrate two of the masses seen on the axial images (A, C). A thick-slab maximum intensity projection image (F) does not demonstrate the two more cephalad lesions.
Diagnosis: Multifocal transitional cell carcinoma
Discussion: Urothelial neoplasms must be strongly considered as the most likely diagnoses (for the focal bladder wall thickening and the three masses) in this patient, although cystitis can occasionally produce masslike bladder abnormalities. The poorly defined intraluminal bladder abnormality located anteriorly on the right may represent a small amount of blood clot.
Up to one-third of bladder cancers are multifocal at the time of diagnosis. For this reason, it is important that the radiologist not give in to satisfaction of search. Careful attention must be paid to the remainder of the bladder once a mass is detected since other masses may be present. Also, patients with bladder cancer must be followed carefully when they are treated without bladder resection since additional cancers or recurrences may develop.
Bladder cancers may not be identified on standard three-dimensional reconstructed images. Lesions can be obscured by densely opacified urine. For this reason, one should not rely exclusively on three-dimensional images for image interpretation. Axial and/or thin section reformatted images should be carefully scrutinized in all patients.
The CT data set can be used to obtain many types of reconstructions, including virtual cystoscopic images. High-quality images can be obtained by utilizing differences in attenuation between the opacified or unopacified portions of the bladder lumen and the adjacent bladder wall or mural masses attached to the bladder wall. These images offer the urologist a view similar to that seen at cystoscopy. Although these views may serve as helpful adjuncts, they do not provide more information than the axial images.
Case 10-5
History: 45-year-old male with gross hematuria.
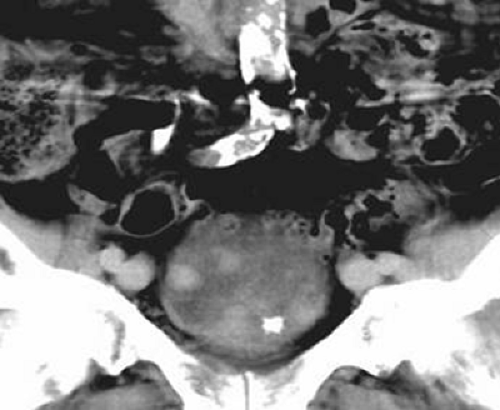 Figure 10.5 A |
 Figure 10.5 B |
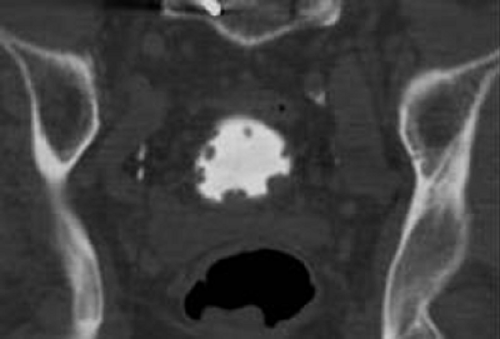 Figure 10.5 C |
 Figure 10.5 D |
Findings: Two thin section (1.25 mm thick) coronal excretory phase images (A, B) are provided of the anterior and posterior aspects of the bladder using standard soft tissue windowing. The second image (B) is also shown using wide windows (C). These images demonstrate multiple mural masses projecting into the bladder lumen. The masses are easily seen, regardless of whether they are surrounded by opacified or unopacified urine, although the lesions along the posterior aspect of the bladder are better seen on the wide window image. These abnormalities are also detected on an average intensity projection image obtained with intermediate (15 mm) thickness (D).
Diagnosis: Multifocal transitional cell carcinoma
Discussion: The differential diagnosis of multiple bladder masses includes both malignant and benign processes. Multifocal transitional cell carcinoma (TCC) is certainly a distinct possibility, although rarely severe chronic cystitis can have a similar appearance. Follow-up cystoscopy is warranted.
This case illustrates the frequent multifocal nature of bladder cancers at the time of detection. Thin section reformatted images have comparable sensitivity in detecting urinary tract pathology to axial images and provide an orientation often preferred by urologists. However, as with axial images, wide windowing (usually using windows of 2,000 to 4,000 HU and levels of 500 to 1,000 HU) is essential to maximize sensitivity in detecting small lesions located adjacent to densely opacified urine. Although three-dimensional reconstructions of thick slabs are insensitive in detecting bladder abnormalities (see Case 10-4), three-dimensional reconstructions of intermediate thickness have intermediate sensitivities. When the findings are extensive, as in this case, reconstructions of intermediate thickness (or less) will usually identify bladder masses.
Case 10-6
History: 68-year-old male with persistent microscopic hematuria. History of prior, successfully treated, superficial bladder cancer and of transurethral resection of the prostate. Recent negative cystoscopy.
 Figure 10.6 A |
 Figure 10.6 B |
 Figure 10.6 C |
Findings: Two axial excretory phase CT urographic images (A, B) through the base of the bladder are provided. The urine in the bladder lumen is homogeneously opacified with excreted contrast material. A small amount of contrast material extends directly posteriorly in the midline, opacifying the defect from the transurethral resection of the prostate. There is asymmetric thickening of the left side of the bladder posteriorly. The interface between the bladder lumen and the bladder wall is slightly irregular. Bilateral inguinal hernias (containing only fat) are also incidentally noted. A maximum intensity projection coronal thick-slab image (C) does not demonstrate the bladder base abnormality.
Diagnosis: Transitional cell carcinoma
Discussion: It is difficult to differentiate prostatic enlargement from a bladder base wall abnormality, with the latter representing either focal changes of cystitis or, more likely, changes from a bladder neoplasm. Clues to the presence of a bladder wall abnormality include an irregular interface between the bladder lumen and wall and asymmetry in the appearance of the bladder lumen and bladder wall (both shown in this case).
Although cystoscopy is considered to be the gold standard for evaluation of the bladder for anatomic abnormalities, there are occasional false-negative cystoscopy results. This is more often true with cancers arising along the anterior wall of the bladder and at the bladder base. It is easy to understand why bladder base cancers may be missed at cystoscopy. Visualization of these neoplasms requires that the cystoscope be angled back upon itself. This may be particularly difficult in patients whose bladder bases are elevated by enlarged prostate glands.
Case 10-7
History: 52-year-old female with one episode of gross hematuria.
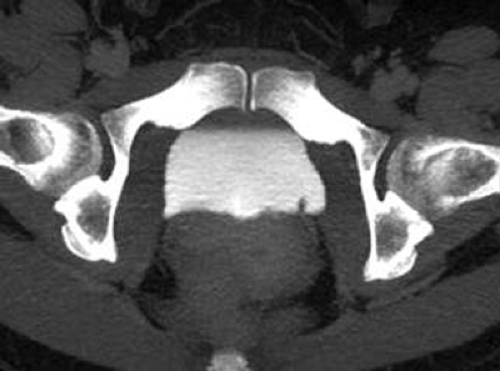 Figure 10.7 A |
 Figure 10.7 B |
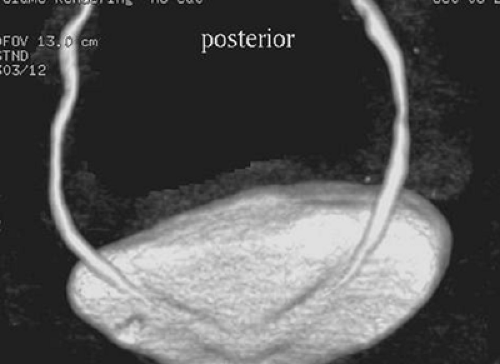 Figure 10.7 C |
Findings: A single excretory phase axial CT urographic image filmed at wide windows (A) demonstrates a tiny 3 mm filling mass along the posterior aspect of the left side of the bladder. A thin section coronal image filmed at wide windows (B) also demonstrates the lesion, along the inferior aspect of the bladder, on the left. In addition, the lesion can also be identified on the posteroanterior volume-rendered image (C) as a small mass just caudal to the left ureterovesical junction. The mass could not be seen on the anteroposterior view.
Diagnosis: Tiny papillary transitional cell carcinoma
Discussion: As with excretory urography, the differential diagnosis for filling defects includes tumor, blood clot, and fungus ball; however, stone is unlikely because nearly all urinary tract calculi are of high CT attenuation (appearing similar to that of contrast-enhanced urine in the bladder lumen on excretory phase CT urographic images). By far the most likely diagnosis in a patient with a single tiny filling defect is urothelial neoplasm.
Tiny urothelial abnormalities can be detected with CT urography. In this instance, the detected lesion can be seen with multiple reconstruction techniques. Use of wide windowing is essential for all images, however, because the tiny lesion would be completely obscured by volume averaging with adjacent densely opacified urine if images were viewed using narrow windows.
Tiny papillary transitional cell carcinomas are often low grade and rarely invade the urothelium. Thus, they can usually be definitely treated (snared and removed) during cystoscopy.
Case 10-8
History: Elderly man with hematuria.
 Figure 10.8 A |
 Figure 10.8 B |
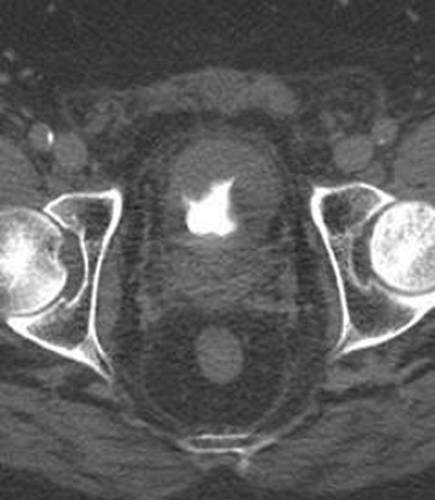 Figure 10.8 C |
Findings: Three excretory phase axial images (A, B and C) from a CT urogram demonstrate marked diffuse bladder wall thickening. The bladder lumen is narrowed and the bladder wall surface irregular.
Diagnosis: Diffuse transitional cell carcinoma
Discussion: Diffuse bladder wall thickening is usually due to either muscular hypertrophy as a result of outlet obstruction, neurogenic bladders, or changes from cystitis. Rarely, bladder cancer can produce diffuse rather than focal wall thickening and can have an appearance indistinguishable from severe changes from the previously described benign entities. In such patients, history and physical examination may facilitate differentiation. Follow-up evaluation with cystoscopy is warranted.
Case 10-9
History: 64-year-old male with positive urine cytology status post treatment of superficial bladder cancer.
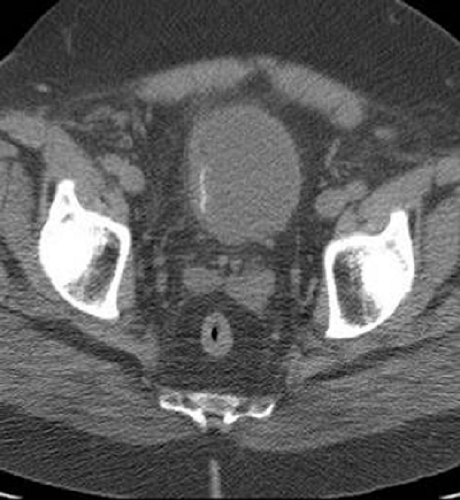 Figure 10.9 A |
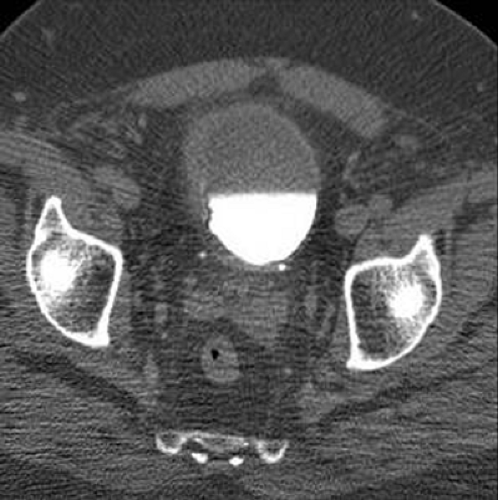 Figure 10.9 B |
Findings: Two axial images from a CT urogram are provided. The first image (A), obtained prior to administration of contrast material, demonstrates a thin rim of linear calcification along the surface of a thickened right lateral wall of the bladder. The second image (B), obtained during the excretory phase after contrast material administration, confirms the presence of focal bladder wall thickening on the right and anteriorly.
Diagnosis: Scarring in right lateral bladder wall and missed cancer in left lateral bladder wall
Discussion: This case illustrates how CT urography can detect many anatomic abnormalities but often cannot distinguish between benign and malignant pathology. Thickening on the right was the result of scarring due to prior local treatment of the superficial bladder cancer. Linear calcification along the bladder wall at this location suggests that the changes were likely chronic and due to scarring. Calcification in bladder cancer is rare and, when present, is often more focal. This case also illustrates that some bladder cancers cannot be detected on CT urography. At cystoscopy, this patient was found to have a superficial cancer along the left lateral wall of the bladder. This neoplasm cannot be identified, even in retrospect. Although it is the opinion of many investigators that CT urography has improved sensitivity in detecting bladder cancers compared to both excretory urography and cystography, it cannot be used to detect all cancers, particularly those that are small or flat.
Case 10-10
History: 57-year-old male with persistent microscopic hematuria.
 Figure 10.10 A |
 Figure 10.10 B |
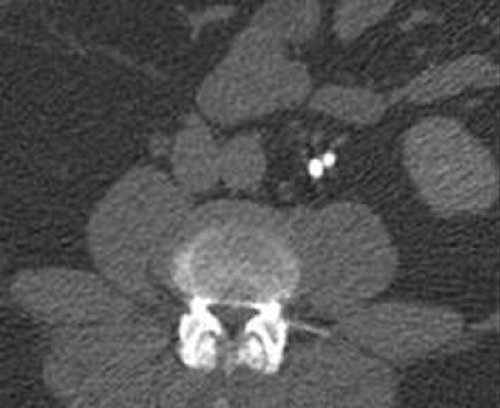 Figure 10.10 C |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


