CHAPTER 5
Colon
INTRODUCTION
The colon can be divided into six segments both anatomically and endoscopically. Unlike in the stomach, the histology of the colon is relatively uniform. These segments can be divided into the cecum, where the ileocecal valve and appendiceal orifice serve as important landmarks; ascending colon; transverse colon; descending colon; sigmoid colon; and rectum. Appreciation of the endoscopic differences between regions is important, particularly when dealing with colonic neoplasms, where accurate localization is essential.
In contrast with the upper gastrointestinal tract, in the colon, diagnosis and therapy of neoplasms assume a prominent role. Although adenomatous polyps are the most frequent neoplastic lesions, a variety of other polyps may masquerade endoscopically; subtle mucosal differences may aid in distinguishing these impostors. Inflammatory disorders such as Crohn’s disease and ulcerative colitis represent another important group of diseases. Other inflammatory disorders, including ischemia and infections (bacterial and viral), assume greater importance in the colon than in the upper gastrointestinal tract. Many of these inflammatory processes appear endoscopically similar; however, differentiation can usually be accomplished based on the characteristics of the patient, location of disease (pancolonic versus segmental), and characteristics of the disease in the involved segment (e.g., circumferential versus patchy; ulcer versus no ulcer).
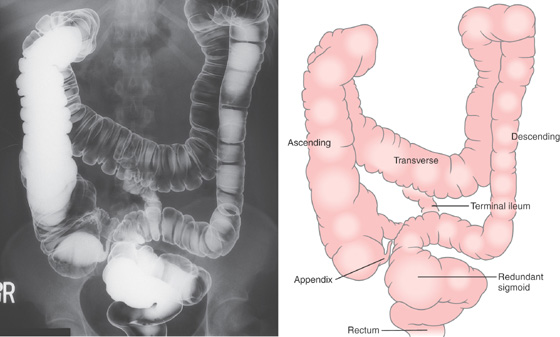
Figure 5.1 BARIUM ENEMA
An air-contrast barium enema demonstrates the normal anatomy of the colon. The sigmoid colon is redundant. The transverse colon dips inferiorly into the pelvis. The ascending and descending colon are retroperitoneal and fixed. The sigmoid and transverse colon have suspending mesentery and are thus mobile. The appendix is filled and seen in the pelvis. Reflux of barium demonstrates the distal terminal ileum.
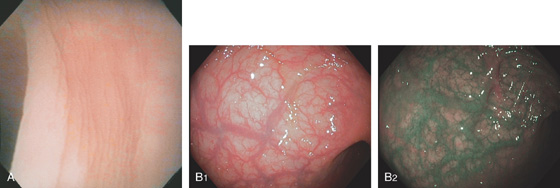
Figure 5.2 NORMAL MUCOSAL PATTERN
A, The normal descending colon visualized underwater demonstrates a linear appearance of the mucosa. B1, The normal colonic mucosal vascular pattern as seen on high-definition endoscopy. B2, The mucosal vascularity is now green when visualized by narrow band imaging.
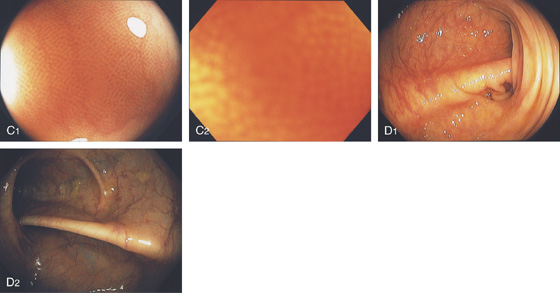
C1, C2, Close-up of the colonic mucosa demonstrates a honeycomb-type pattern. D1, At the flexures, one can oftentimes see the longitudinal colonic muscle, or teniae, which provides the direction of the lumen (D2).
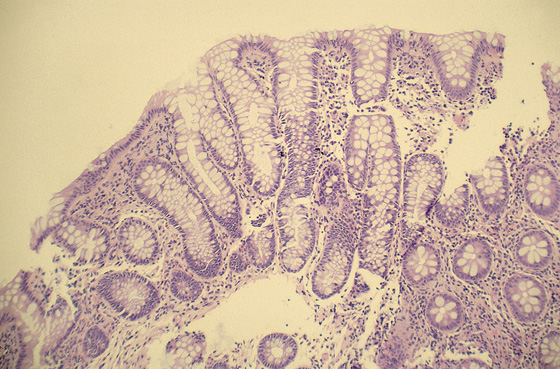
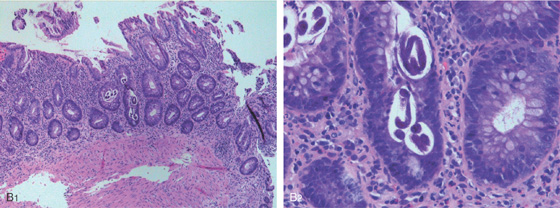
Figure 5.3 HISTOLOGY
Normal colonic architecture. The crypts form the multiple round structures seen in cross section.
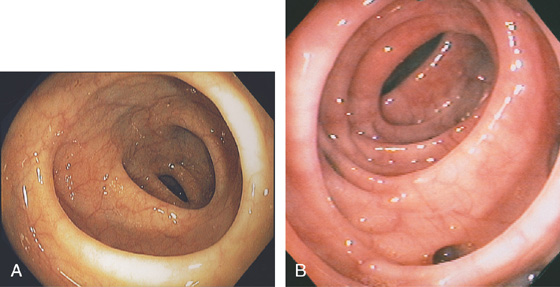
Figure 5.4 SIGMOID COLON
A, Circular folds of modest thickness are identified. B, The sigmoid colon demonstrates thickened circular folds corresponding to hypertrophied musculature. Several diverticula are present.
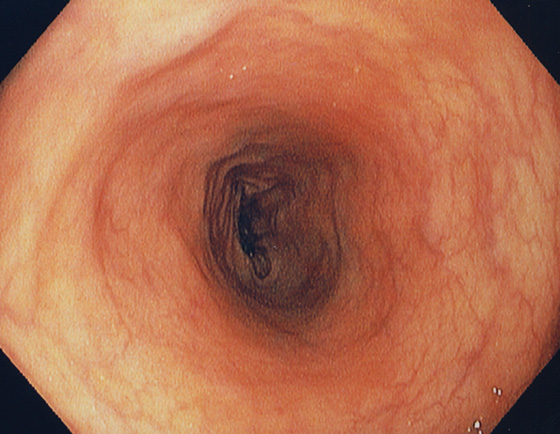
Figure 5.5 DESCENDING COLON
The descending colon forms a long tube and is relatively featureless.
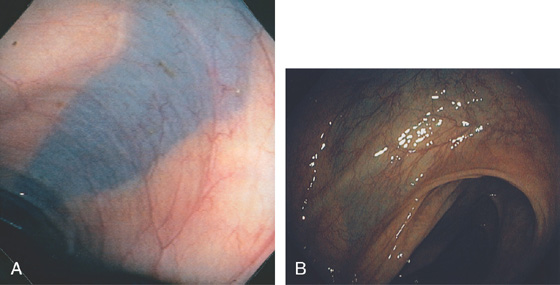
Figure 5.6 SPLENIC FLEXURE
A long, bluish indentation from the spleen. Normal colonic vasculature is seen. A, Long bluish indentation from the spleen, with normal overlying colonic vasculature. B, Dark area easily identified under a normal colonic vascular pattern.
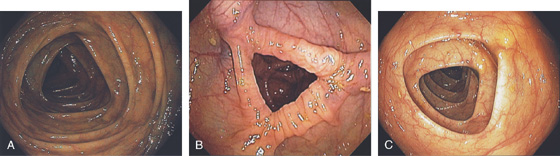
Figure 5.7 TRANSVERSE COLON
A-C, The typical-appearing triangular folds of the transverse colon.
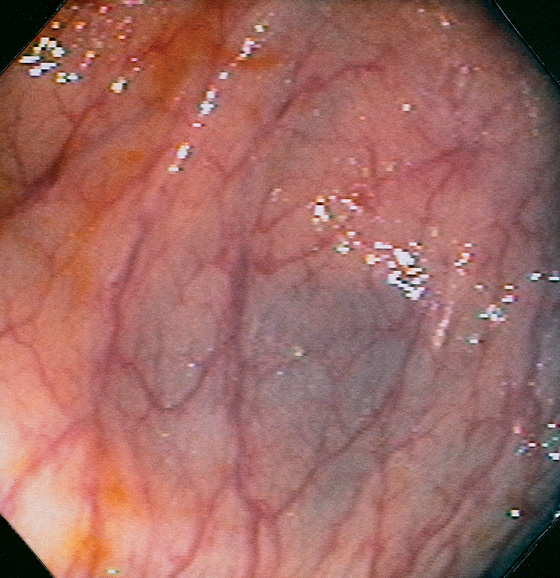
Figure 5.8 HEPATIC FLEXURE
The hepatic flexure is noted by the darkish hue from the liver. Normal colonic vasculature is seen overlying the bluish hue of the liver. Visualization of the adjacent liver will depend on the position of the patient.
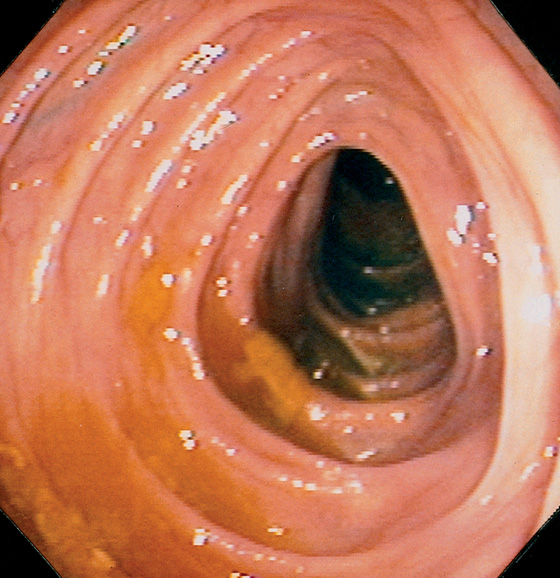
Figure 5.9 ASCENDING COLON
The ascending colon may also have triangular folds. The ileocecal valve is in the distance.
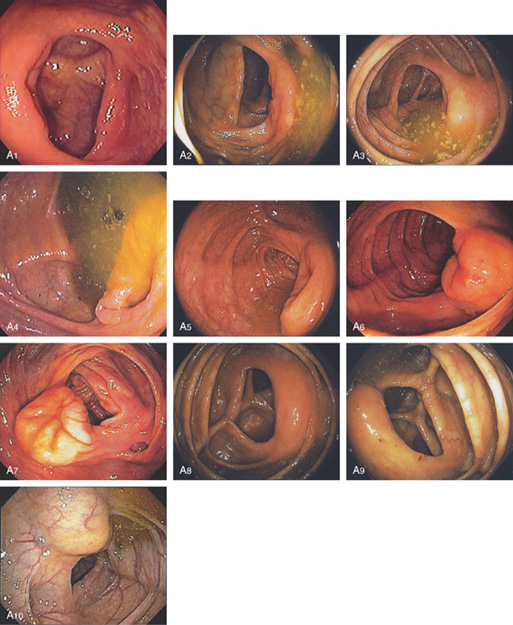
Figure 5.10 ILEOCECAL VALVE
A, Appearance of a normal ileocecal (IC) valve (A1-A10). Note that fluid in the right colon puddles by the IC valve when the patient is in the left lateral decubitus position regardless of the rotation of the endoscope and can be used as a landmark.

Figure 5.11 CECAL POLE
The slit of the appendiceal orifice resides at the base of the cecal pole. Folds radiate from the base of the cecum to the transverse cecal fold.
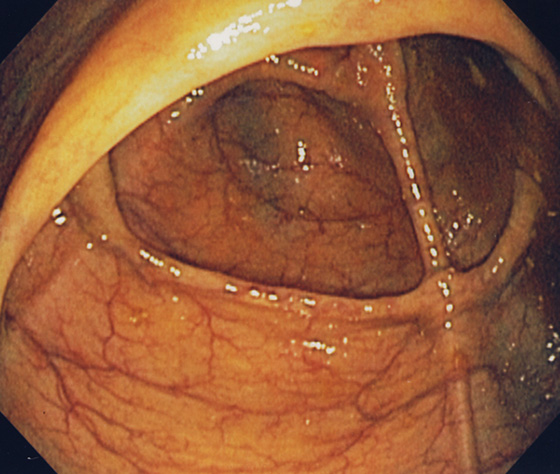
Figure 5.12 CECUM
The thickened yellow structure represents the ileocecal valve. On the contralateral wall, the thickened tinea coli converge with several others forming the transverse cecal fold, “crow’s foot” or cecal strap.
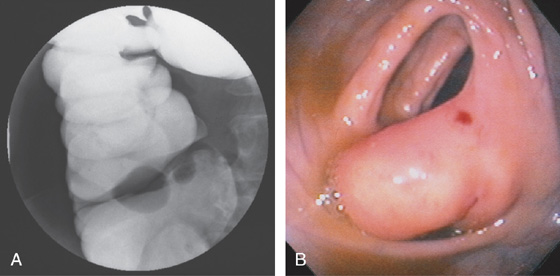
Figure 5.13 LIPOMATOUS ILEOCECAL VALVE
A, A smooth filling defect extending from the medial wall at the level of the ileocecal valve. B, The filling defect represents a bulbous (fatty) ileocecal valve. The red area on the fatty valve resulted from endoscopic trauma.
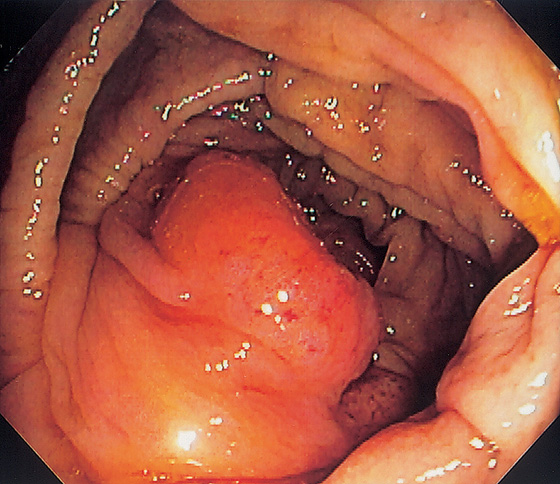
Figure 5.14 PROLAPSED ILEOCECAL VALVE
Masslike appearance from prolapse of the valve. Biopsy confirmed ileal epithelium.
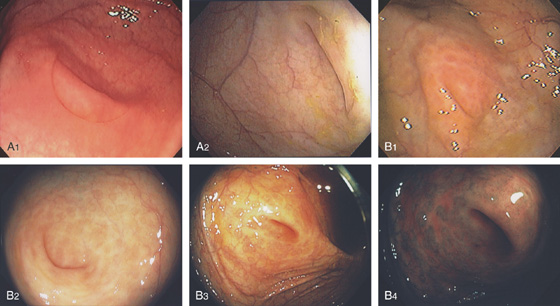
Figure 5.15 APPENDICEAL ORIFICE
A1, A2, Slitlike semilunar structure at the base of the cecum. B1, B2, Slitlike opening at the base of the cecum. The “leopard skin” pattern around the appendiceal orifice represents lymphoid follicles that are frequently identified in the cecal pole. B3, B4
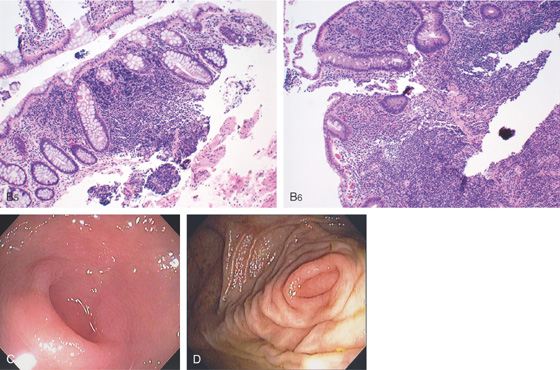
Narrow band imaging highlights the lymphoid follicles (B5, B6). C, Circular raised area at the base of the cecum. The appendiceal orifice is at the base of this structure. D, Multiple circular folds surround the appendiceal orifice.

Figure 5.16 EVERTED APPENDIX
A1, Circular folds emanating from an indentation in the cecal pole. A2, With further observation, the appendix was seen to spontaneously evert, simulating a polyp. B, Fleshy tissue emanating from the base of the cecum.
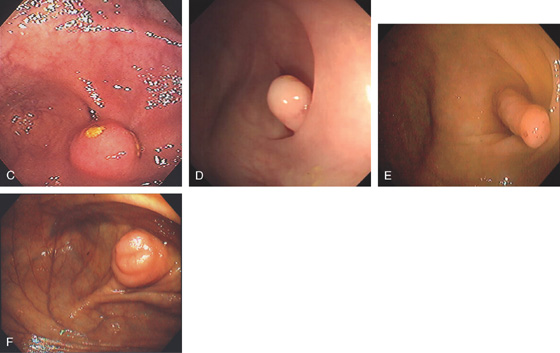
C, Round, submucosal-appearing lesion at the base of the cecum with overlying exudate. This patient had a prior appendectomy. D, Short finger-like projection from the base of the cecum resembling a pedunculated polyp. E, Long finger-like projection from the base of the cecum resembling a pedunculated polyp. F, Round polypoid lesion at the base of the cecum resembling a sessile polyp.
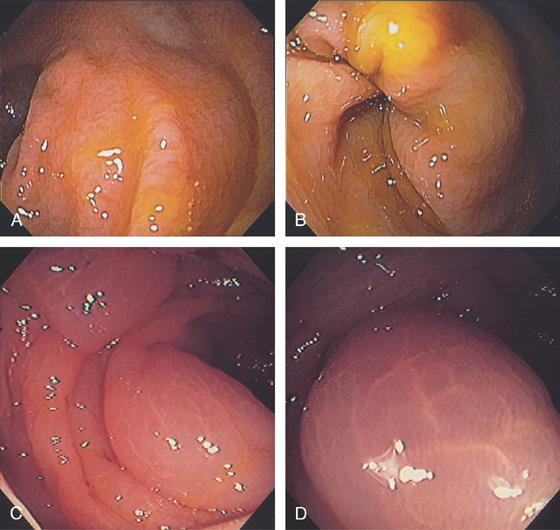
Figure 5.17 COLONIC EDEMA
A, B, Mild colonic edema highlights the normal mucosal pattern. C, Marked edema of the colon with loss of vascular pattern. D, Close-up shows the accentuated architecture of the mucosal pattern.
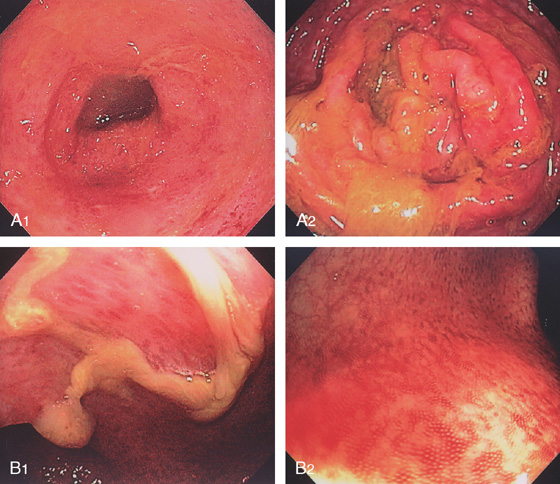
Figure 5.18 ACUTE CULTURE-NEGATIVE BACTERIAL COLITIS
A1, Edema, loss of vascular pattern, subepithelial hemorrhage, and exudate in the descending colon. A2, Stool and pus are in the ascending colon. B1, Diffuse subepithelial hemorrhage with thick mucopus. B2, Striking subepithelial hemorrhage of the distal colon. Note the subepithelial hemorrhage spares the lymphoid follicles, creating a honeycomb pattern.
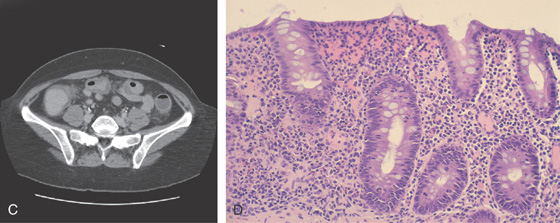
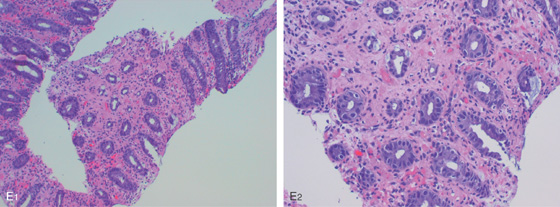
C, Pancolitis with circumferential wall thickening in each segment. The bowel wall thickening is accentuated by the fluid-filled colon. Note the inflammatory process (stranding) extends around the colon, most striking in the cecum and descending colon. D, The colonic mucosa has both an acute and a chronic inflammatory infiltrate and mild cryptitis. The crypt architecture is preserved, suggesting acute rather than chronic colitis.
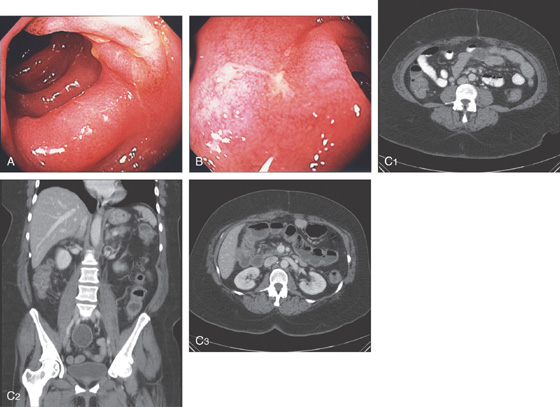
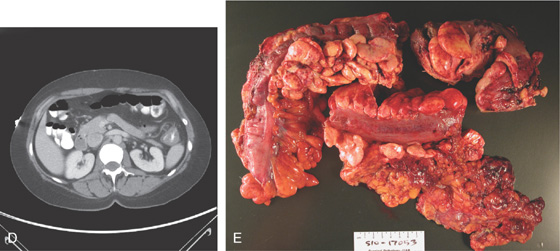
Figure 5.19 SALMONELLA COLITIS AND ILEITIS
A, Edema, granularity, and mucopus are in the sigmoid colon. B, Similar findings are present in the ileum. C1, C2, The colon is mildly edematous. The colon wall enhances with intravenous contrast injection. There is mild thickening of the left colon (C3).
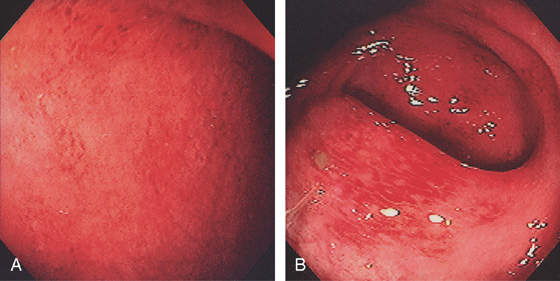
Figure 5.20 CAMPYLOBACTER COLITIS
A, Diffuse erythema with patchy subepithelial hemorrhage in the distal colon. Stool culture was positive for Campylobacter jejuni. B, A small ulcer surrounded by subepithelial hemorrhage is shown more proximally.
![]() Differential Diagnosis
Differential Diagnosis
Campylobacter Colitis (Figure 5.20)
Inflammatory bowel disease, ulcerative colitis
Ischemia
Other infections (bacterial, viral)
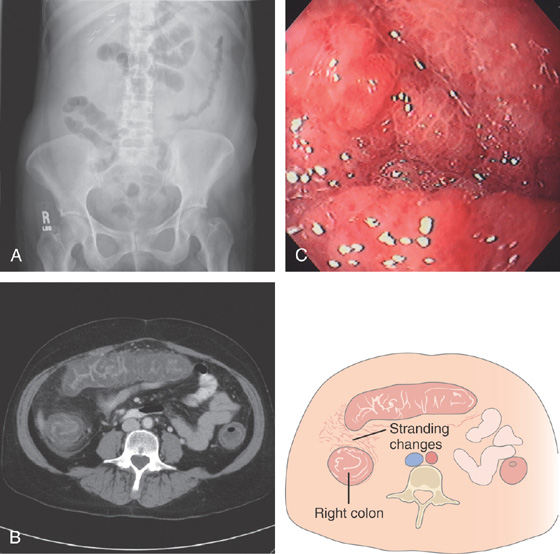
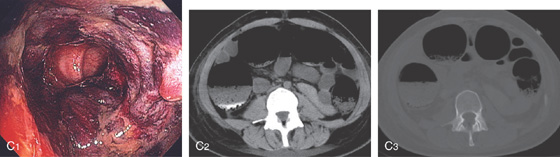
Figure 5.21 ESCHERICHIA COLI 0157 H7
A, Thumbprinting and luminal narrowing of the distal transverse colon. B, Pancolitis with mucosal enhancement. Note the stranding changes around the right colon. C, Diffuse edema and subepithelial hemorrhage of the distal colon. Stool culture was positive.

Figure 5.22 CLOSTRIDIUM DIFFICILE COLITIS
A1, A2, Characteristic multiple circular, plaquelike lesions of the distal colon. Note the halo of erythema and the loss of vascular pattern in the surrounding mucosa. B, Diffuse erythema and edema of the distal colon with overlying exudate.
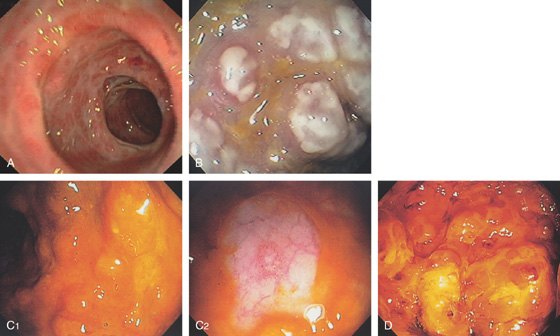
Figure 5.23 CLOSTRIDIUM DIFFICILE COLITIS
A, Patchy circular subepithelial hemorrhage in the distal colon. There is colonic edema with loss of the normal mucosal vascular pattern. B, Multiple raised white plaquelike lesions. C1, Multiple nodules underneath a thin coating of stool. C2, Washing of the lesions demonstrates pinpoint erosions. D, Multiple bullae of the distal colon.
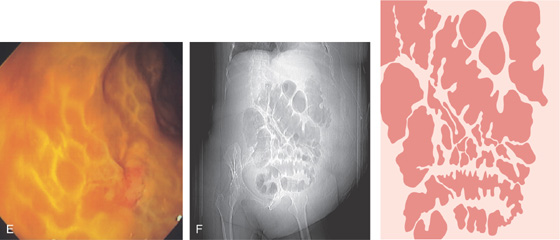
E, Severe edema with overlying exudate. The honeycomb appearance of the mucosa is apparent and is caused by the marked edema. F, Thumbprinting is apparent.
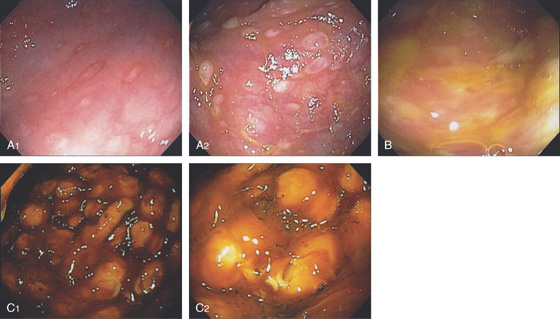
Figure 5.24 CLOSTRIDIUM DIFFICILE COLITIS
A1, Patchy, well-circumscribed areas of erosion with surrounding hyperemia. A2, More proximally, the colitis becomes more severe and the typical pseudomembranes are observed. B, Flat pseudomembranes with areas of mucopus. C1, Multiple pseudomembranes have a nodular appearance. C2, No normal mucosa can be appreciated.
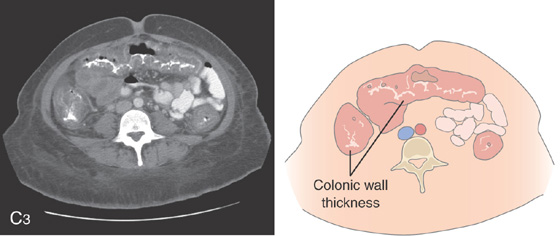
C3, Striking colonic wall thickness is present.
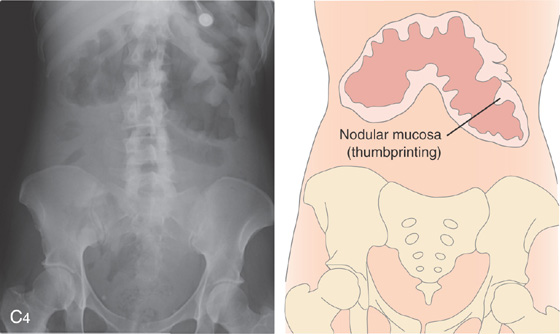
Note the nodular mucosa can also be seen on kidneys, ureter, and bladder termed thumbprinting (C4).
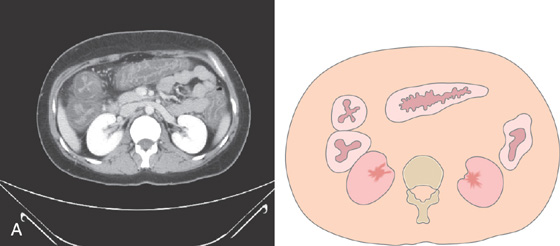
Figure 5.25 CLOSTRIDIUM DIFFICILE COLITIS
A, Diffuse thickening of the entire colon with contrast enhancement of the mucosa.
B, Severe colitis with acute and chronic inflammatory cells and edema. A mushroom-shaped pseudomembrane is shown. The colonic architecture is preserved.
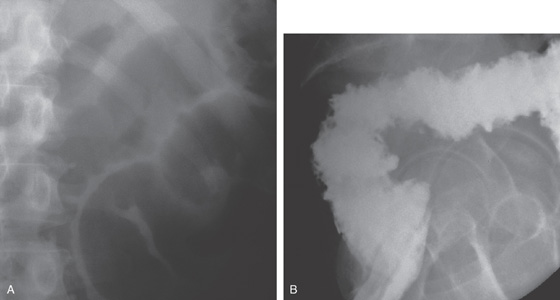
Figure 5.26 SEVERE CLOSTRIDIUM DIFFICILE COLITIS
A, Abdominal radiograph shows subtle nodularity of the colon. B, Marked irregularity of the rectal wall.
C, The more proximal colon demonstrates marked nodularity (thumbprinting) of the wall. The mucosa in some areas is poorly coated by the barium. D, The colonic wall is covered by a thick, tenacious membrane. The rectum had multiple well-circumscribed yellow plaques characteristic of C. difficile colitis.
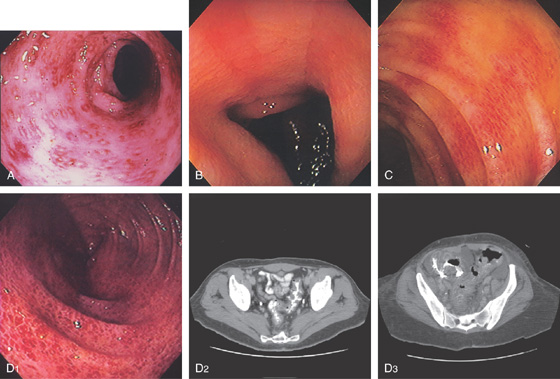
Figure 5.27 CYTOMEGALOVIRUS COLITIS
A, Multiple small, well-circumscribed, ringlike lesions with surrounding subepithelial hemorrhage. There is a diffuse colitis. B, Edema and erythema of the sigmoid colon. C, Prominent subepithelial hemorrhage of the descending colon. D1, Striking diffuse subepithelial hemorrhage. D2, Diffuse colonic wall thickening from rectum to right colon (D3).
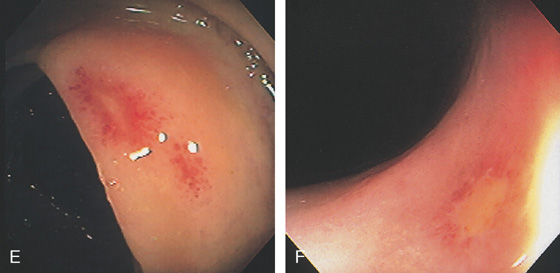
Figure 5.27 CYTOMEGALOVIRUS COLITIS
E, Well-circumscribed small ulcer with a halo of erythema and subepithelial hemorrhage. F, Flat ulcer with normal surrounding mucosa.
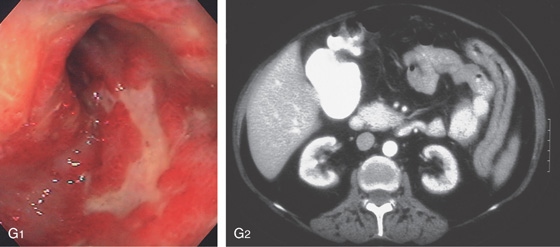
G1, Serpiginous ulcers in the rectum with an appearance suggestive of Crohn’s disease. G2, Marked thickening of the left colon.
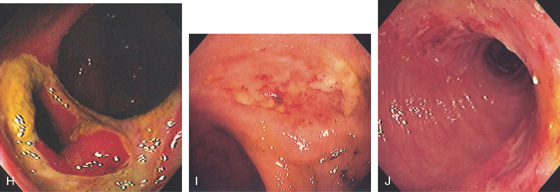
H, Large ulcer of the cecum involving the ileocecal valve. I, Large shallow ulcer with exudate. J, Hemicircumferential ulceration at an ileocolonic anastomosis.
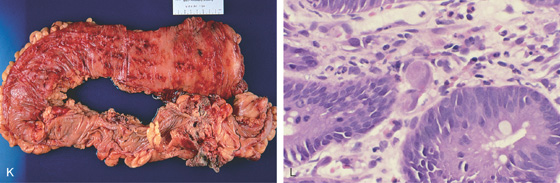
K, Diffuse petechial lesions throughout the left colon. L, Enlarged endothelial cell containing cytomegalovirus inclusions. A moderate amount of chronic inflammation is in the lamina propria.
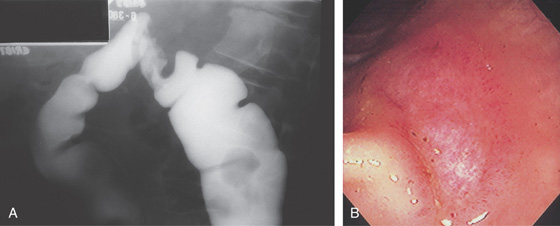
Figure 5.28 CYTOMEGALOVIRUS COLITIS
A, Barium enema shows a focal defect at the splenic flexure suggestive of neoplasm. B, Well-circumscribed ulceration with surrounding edema.
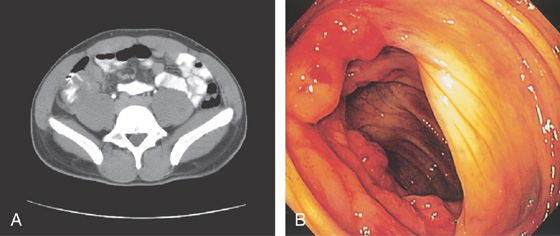
Figure 5.29 TUBERCULOUS COLITIS
A, Thickening of cecum. B, Marked nodularity and fresh hemorrhage around the ileocecal valve.
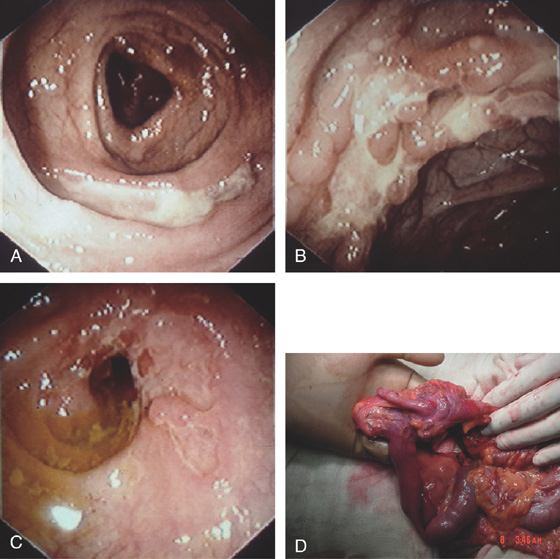
Figure 5.30 TUBERCULOUS COLITIS
A, Focal ulceration of the sigmoid colon. B, Serpiginous ulceration of the right colon. C, Circumferential ulceration with formation of a stricture. D, Marked stricturing of the cecum.
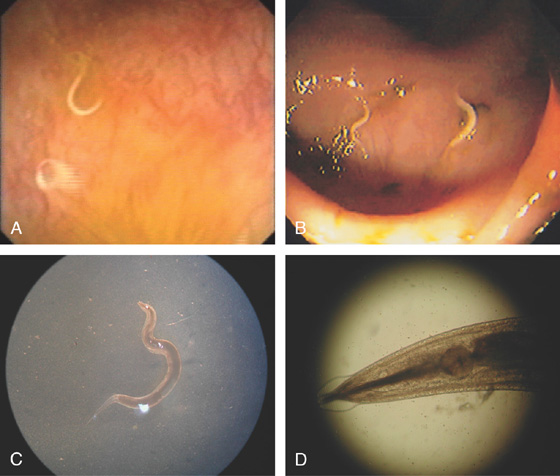
Figure 5.31 PINWORM INFECTION (ENTEROBIUS VERMICULARIS)
A, Solitary worm. B, Multiple small worms in the cecum characteristic of pinworms. C, D, Under the microscope, unique features of the worm are better appreciated.
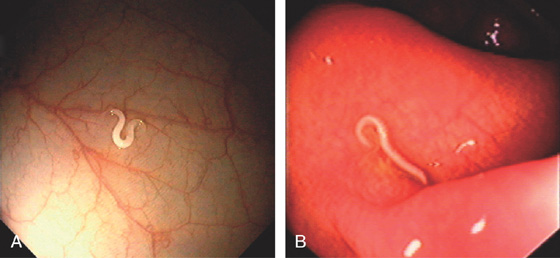
Figure 5.32 WHIPWORM INFECTION (TRICHURIS TRICHIURA)
Solitary worms (A, B).
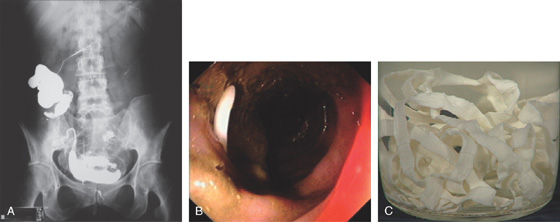
Figure 5.33 TAPEWORMS (TAENIA SPECIES)
A, Barium study shows worm in the cecum and ascending colon, as well as transverse colon. B, The worm appears as white object in the stool. C, The length of the worm is apparent after removal.
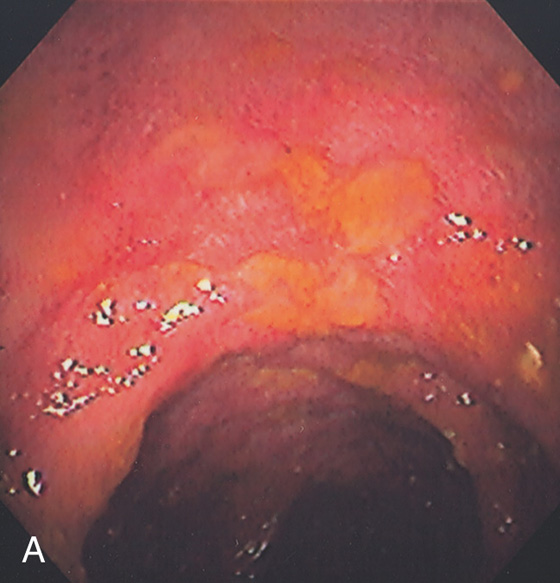
Figure 5.34 STRONGYLOIDES COLITIS
A, Marked colonic edema with patchy shallow ulceration.
B1, Low-power view shows acute colitis with structures present in the crypts. B2, High-power view shows larvae in the crypts.
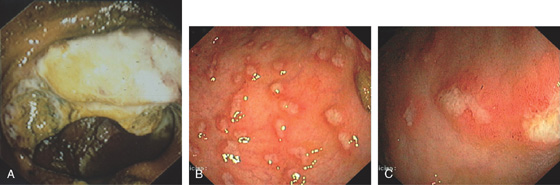
Figure 5.35 AMEBIC COLITIS
A, Large ulcer involving the ileocecal valve. Ulceration is also present in the cecum. B, Patchy well-circumscribed ulcers. C, Close-up shows the ulcers having a raised (volcano) appearance.
![]() Differential Diagnosis
Differential Diagnosis
Amebic Colitis (Figure 5.35)
Inflammatory bowel disease
Other infections (viral, bacterial)
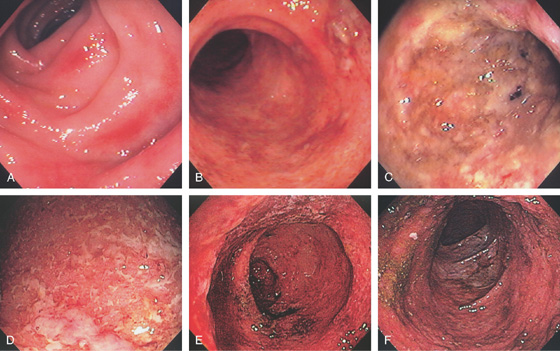
Figure 5.36 ULCERATIVE COLITIS
A, Mild ulcerative colitis demonstrated by edema, loss of the normal mucosal vascular pattern, and patchy subepithelial hemorrhage. B, Moderate colitis with loss of vascular pattern, subepithelial hemorrhage, and patchy mucopus. C, Diffuse mucopus coating the colon. D, Diffuse colitis with diffuse shallow ulceration. E, Diffuse colonic hemorrhage. F, Focal colitis with point of demarcation to normal mucosa.
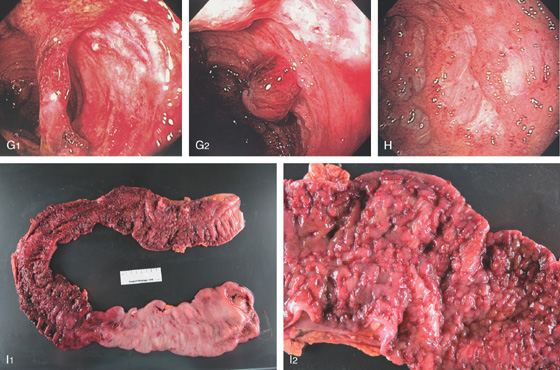
Figure 5.36 ULCERATIVE COLITIS
G1, Severe colitis with mucosal bridge. G2, Deep ulceration with a residual round area of preserved but hemorrhagic mucosa. H, Severe colitis with deep serpiginous ulcerations most suggestive of Crohn’s disease. I1, I2, Surgical specimen shows severe colitis with sparing of cecum.
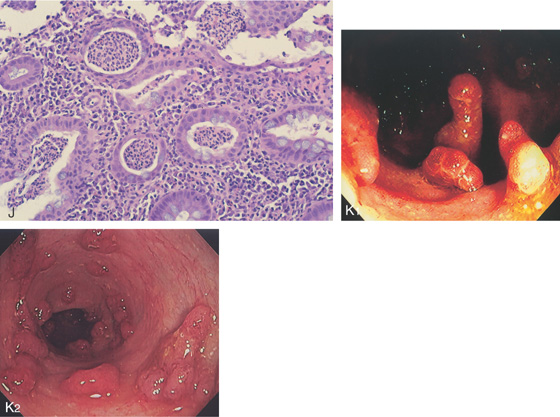
J, Severe acute and chronic inflammatory process, with multiple crypt abscesses. K1, K2, Multiple filiform polyps in the setting of active colitis.
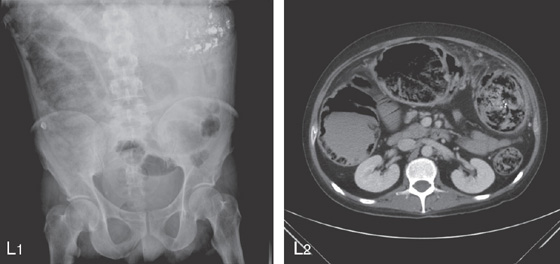
Figure 5.36 ULCERATIVE COLITIS
SEVERE ULCERATIVE COLITIS
L1, Kidneys, ureter, and bladder x-ray film shows haziness in the right colon compatible with pneumatosis. Also note the barium at the splenic flexure. L2, CT scan shows diffuse dilatation of the colon with air not only in the lumen but in the colonic wall.
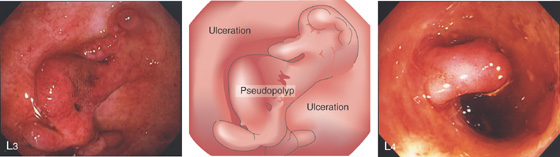
L3, Severe ulceration with mucosal loss and formation of pseudopolyps. L4, Pseudopolyp formation with surrounding ulceration.
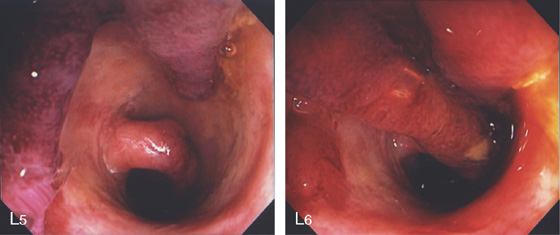
L5, The exudate is removed showing the underlying edema of the mucosa. L6, Formation of long pseudopolyps.
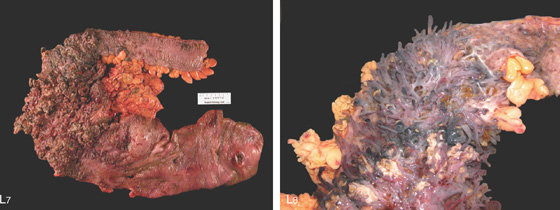
Figure 5.36 ULCERATIVE COLITIS
L7, Surgical specimen shows diffuse colitis, a cecal ulcer, and the marked pseudopolyposis (L8).
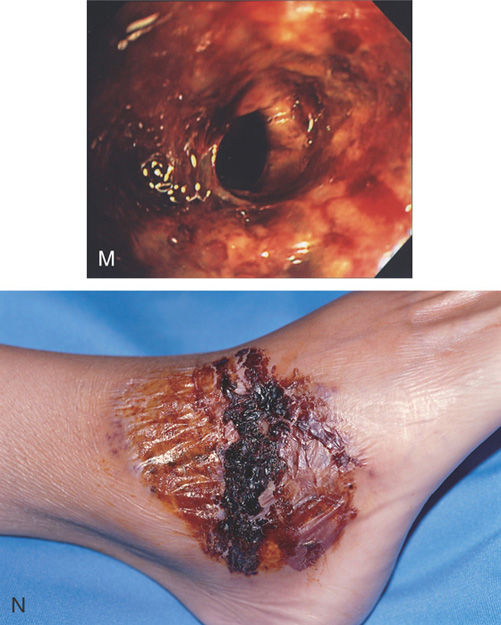
M, Severe ulceration with scarring and luminal narrowing. N, Lesion on the right ankle typical for pyoderma gangrenosum.
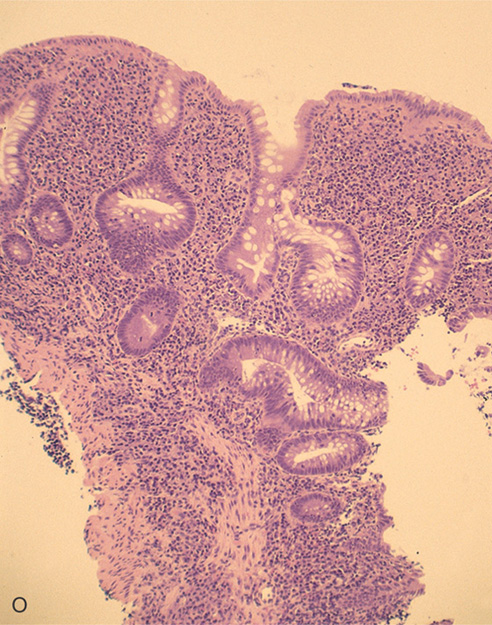
O, The colonic architecture is distorted, with a loss of crypts and abnormal branching of the crypts. The disordered architecture is useful in differentiating acute from chronic colitis.
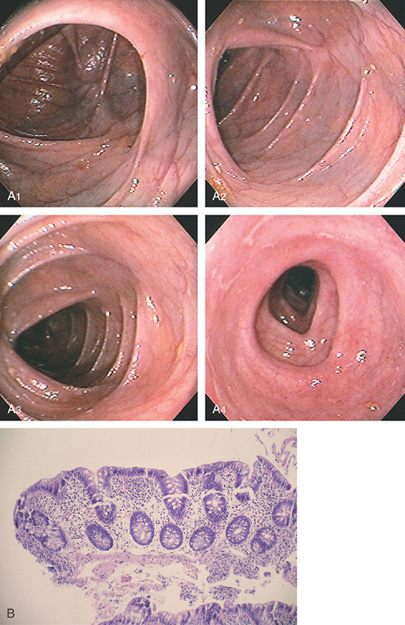

Figure 5.37 ULCERATIVE COLITIS
A, Surveillance colonoscopy in a patient with chronic ulcerative colitis. The ascending colon (A1), transverse colon (A2), and descending colon (A3) are normal, with active disease of the sigmoid colon (A4). B, Biopsy samples of the normal-appearing colon demonstrate abnormal architecture consisting of shortened crypts but no active colitis. C1, C2, Surveillance endoscopy shows mild granularity of the mucosa. The granularity and mild edema are more pronounced in the sigmoid colon (C3).
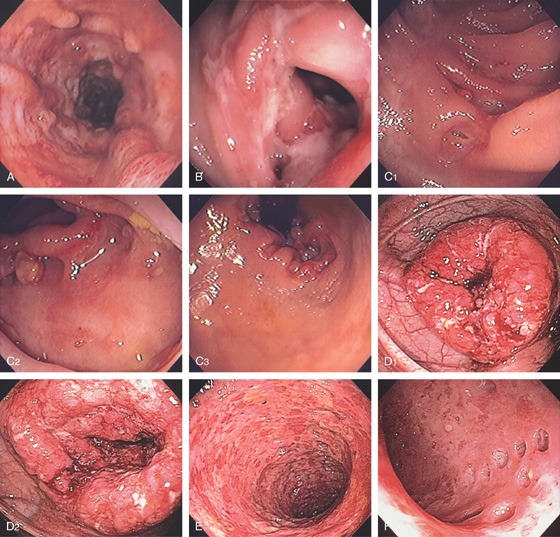
Figure 5.38 COLONIC CROHN’S DISEASE
A, Diffuse deep ulceration with a nodular appearance. B, Focal area of ulceration with distortion, luminal narrowing, and an early fistula. C1, Focal ulceration with an appearance of the ulcer burrowing underneath the mucosal fold. C2, More proximally a large deep ulcer was present, again with the appearance of the ulcer burrowing underneath the mucosa. C3, Marked involvement of the anorectum was present. D1, Focal area of severe colitis resembling a mass lesion in the right colon. D2, Proximally diffuse disease was evident. E, Circumferential ulceration of the distal colon resembling ulcerative colitis. F, Multiple punched-out ulcers with colitis.
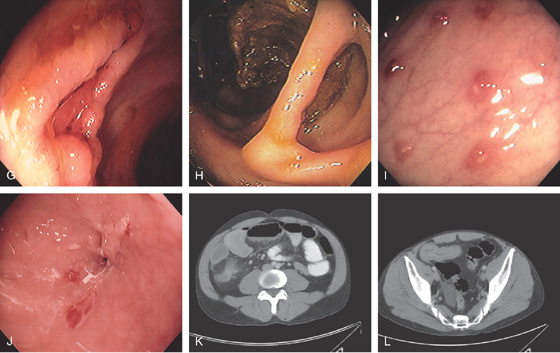
Figure 5.38 COLONIC CROHN’S DISEASE
G, Serpiginous ulcer. H, Mucosal bridge representing healing of a submucosal ulcer. I, Multiple aphthous ulcers. J, Pinpoint area in the distal colon representing a fistulous tract. K, Thickening with inflammatory changes (stranding) around the cecum. L, Thickened terminal ileum.
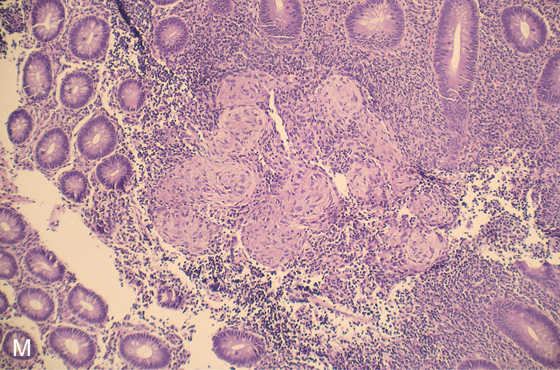
M, Multiple well-circumscribed, noncaseating granulomata. This finding supports the diagnosis of Crohn’s disease when an infectious cause is excluded.
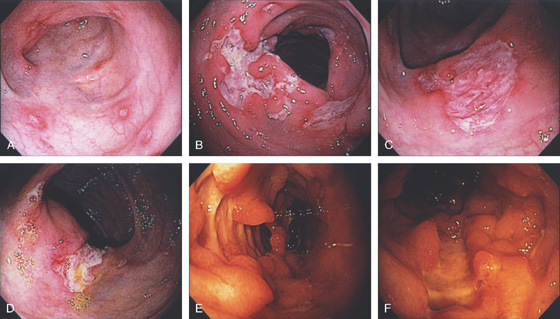
Figure 5.39 COLONIC CROHN’S DISEASE
A, Multiple punctate ulcers in the descending colon. B, Large serpiginous ulceration of the descending colon. C, Solitary ulcer in transverse colon. D, Irregular ulceration involves the ileocecal valve. E, Deep ulceration with associated pseudopolyps. F, “Bear claw”-type ulceration.
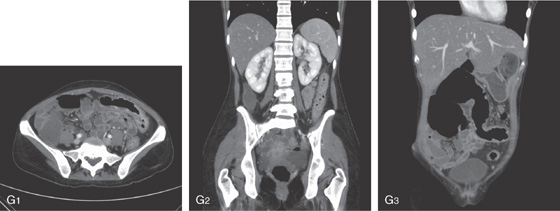
G1-G3, Routine and coronal CT images shows thickened colon. Coronal image shows colonic dilatation and colonic wall thickening.
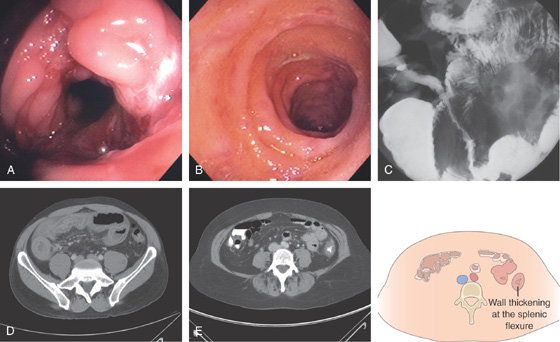
Figure 5.40 ILEOCECAL CROHN’S DISEASE
A, The ileocecal valve is patulous from involvement with Crohn’s disease. The valve is diffusely ulcerated and hemorrhagic. B, The terminal ileum is edematous and hemorrhagic, and has scattered ulcerations typical of Crohn’s ileitis. C, The terminal ileum appears nodular and narrowed (“string sign”). D, CT shows thickening of the right colon and pronounced thickening of a long segment of terminal ileum. E, There is also circumferential wall thickening at the splenic flexure.
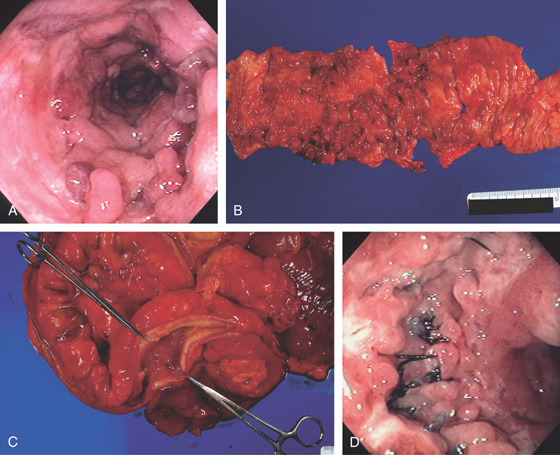
Figure 5.41 COLONIC CROHN’S WITH PSEUDOPOLYPS
A, Diffuse edema, ulceration, and multiple pseudopolyps. B, The surgical specimen demonstrates a normal-appearing colon on the right. The involved area shows ulceration and diffuse polyposis representing inflammatory polyps. C, The surgical specimen demonstrates marked thickening of the colonic wall typical of Crohn’s disease. D, Recurrence at the anastomosis, with deep ulceration surrounding the sutures.
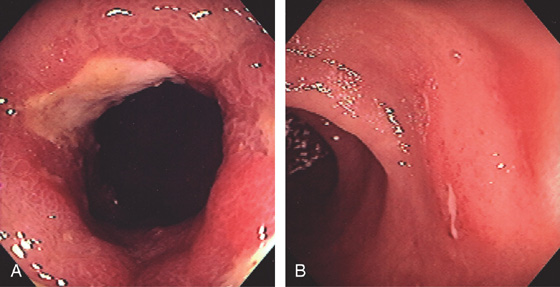
Figure 5.42 RECURRENT CROHN’S DISEASE WITH ANASTOMOTIC ULCER
A, Narrowing, edema, and ulceration at the site of a prior ileocolonic anastomosis. B, Typical serpiginous ulcer seen in the distal ileum just proximal to the anastomosis.
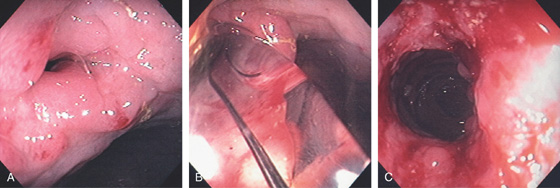
Figure 5.43 ANASTOMOTIC STRICTURE
A, Tight stricture at the site of a prior ileocolonic anastomosis. B, A balloon has been placed across the anastomosis and inflated. C, Improved luminal caliber after dilation.
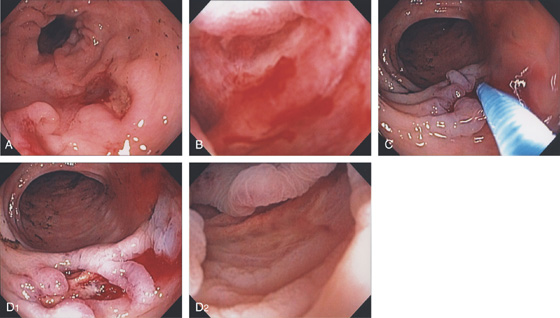
Figure 5.44 COLONIC CROHN’S WITH ULCER-RELATED BLEEDING
A, Deep serpiginous ulceration in the descending colon. B, The ulcer base is viewed underwater showing pinpoint mucosal oozing. C, Epinephrine is injected into the lesion, resulting in blanching of the mucosa and hemostasis (D1, D2).
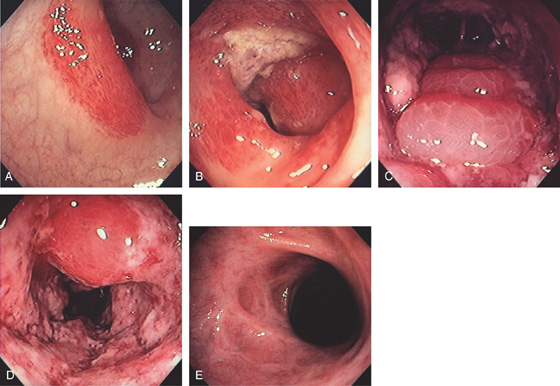
Figure 5.45 ISCHEMIC COLITIS
A, Distinct demarcation manifested by focal subepithelial hemorrhage. B, Proximally, the hemorrhage becomes confluent with ulceration. C, Marked edema of the mucosa forming subepithelial blebs. D, More marked ulceration, edema, and luminal narrowing. E, Follow-up colonoscopy 2 months later shows scarring and distortion.
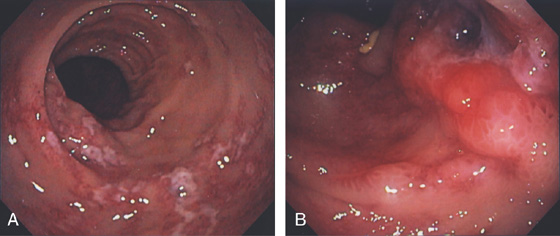
Figure 5.46 ISCHEMIC COLITIS
A, Patchy exudate overlying ulceration in the descending colon. B, More proximally, the ulceration becomes confluent and a deep ulceration with raised border is seen.
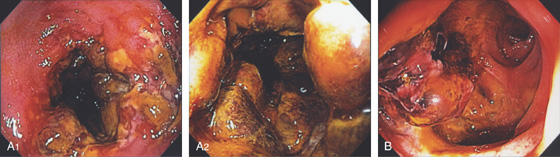
Figure 5.47 ISCHEMIC COLITIS WITH BLEEDING
A1, A2, The ulceration becomes confluent and nodular with marked luminal narrowing. Mucosal biopsy of such a lesion is generally firm with ischemic colitis. B, Large ulceration with fresh bleeding and an adherent blood clot.
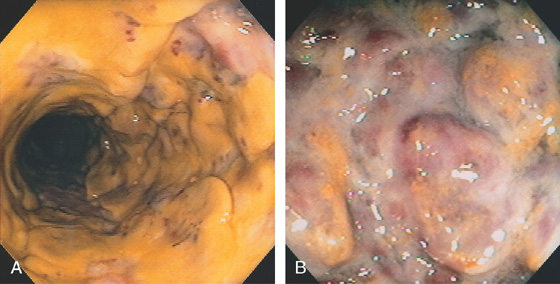
Figure 5.48 ISCHEMIC COLITIS
A, Circumferential ulceration with a thick membrane, resembling Clostridium difficile colitis. B, Marked nodularity and ulceration.
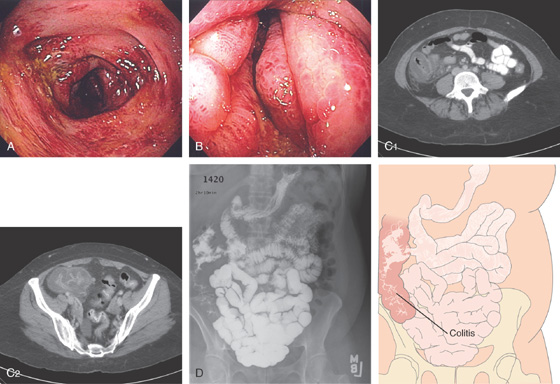
Figure 5.49 RIGHT-SIDED ISCHEMIC COLITIS
A, B, Marked edema and subepithelial hemorrhage of the right colon. The cecum is markedly edematous with luminal narrowing. C1, C2, CT shows edema of the right colon. D, Small-bowel follow-through shows a normal small bowel, but edema of the right colon.
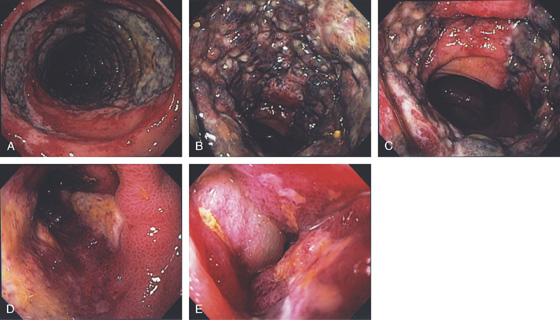
Figure 5.50 ISCHEMIC PROCTITIS
A, Edema of the proximal rectum with circumferential disease. B, Circumferential disease with nodularity and luminal narrowing. C, Note the ulceration stops relatively abruptly, typical for ischemia. D, E, Progression over time shows marked edema.
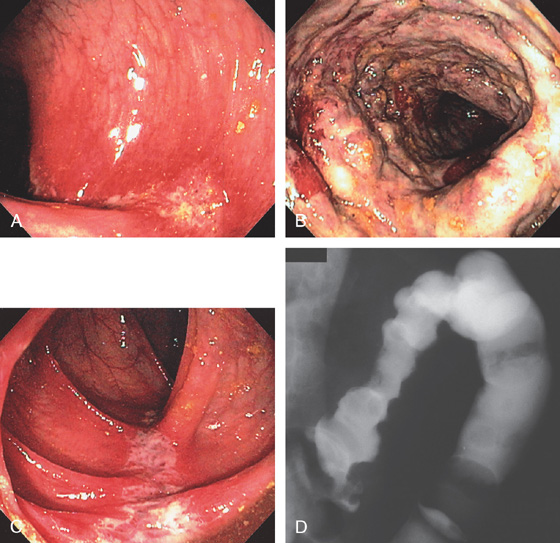
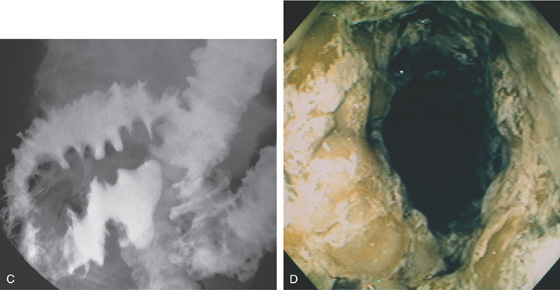
Figure 5.51 ISCHEMIC COLITIS
A, Focal ulceration with surrounding erythema and subepithelial hemorrhage just distal to the splenic flexure. B, More proximally, there is marked edema, ulceration, and subepithelial hemorrhage typical for ischemic colitis. The mucosa was firm on biopsy, also characteristic of ischemic colitis. C, More proximally in the distal transverse colon, the ulceration again follows the tinea with surrounding focal edema. D, Barium enema shows nodularity at the splenic flexure.
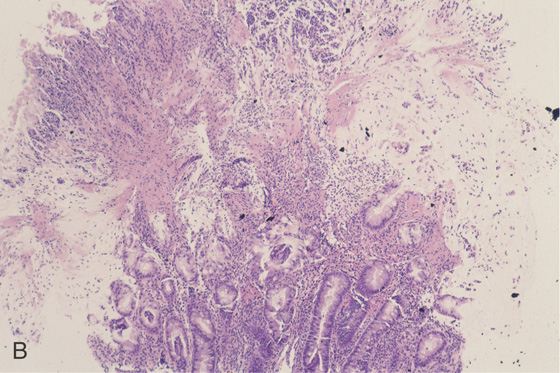
E1, E2, Dropout of glands with fibrosis of lamina propria.
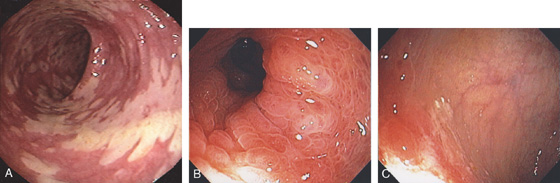
Figure 5.52 ISCHEMIC COLITIS
A, Patchy yellow exudate in the distal colon resembling Clostridium difficile colitis. B, Circumferential edema with a prominent mucosal pattern. C, Abrupt termination of ischemic colitis is characteristic.
D, Colonic thickening at the splenic flexure. E, Resection specimen shows the marked thickening of the colonic wall.
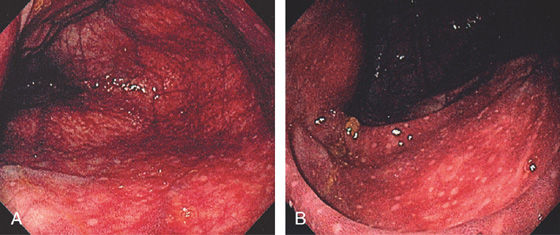
Figure 5.53 ISCHEMIC COLITIS
A, Marked diffuse subepithelial hemorrhage involving the cecum. B, Note the lymphoid aggregates are spared.
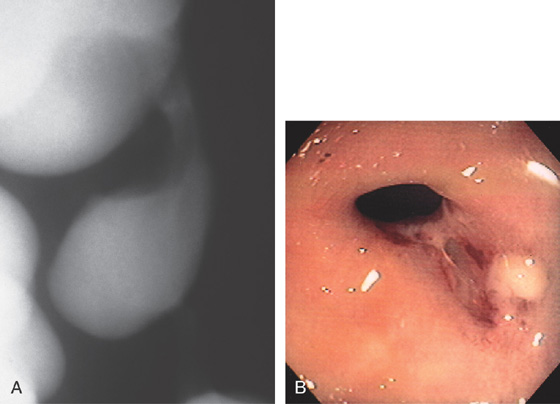
Figure 5.54 ISCHEMIC COLITIS STRICTURE
A, Focal smooth stricture at the splenic flexure. B, Narrowing of the colonic lumen with ulceration at the site of a prior episode of ischemia.
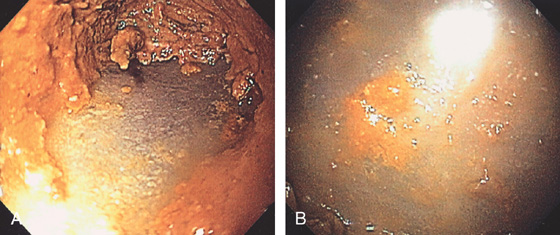
Figure 5.55 INFARCTED COLON
A, Stool coats a black colon. B, Close-up shows the dark discoloration with the absence of normal-appearing mucosa.
C1, Dusky appearance of the distal colon. C2, Air in the right colon wall best appreciated on bone windows (C3).
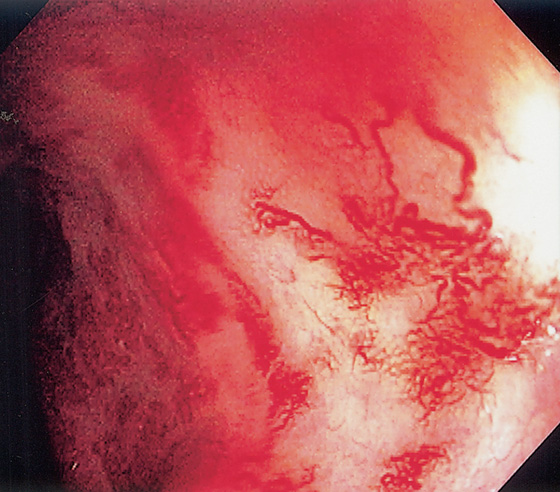
Figure 5.56 RADIATION PROCTOPATHY
Multiple ectatic blood vessels in the distal rectum. This patient previously underwent radiation therapy for prostate cancer.
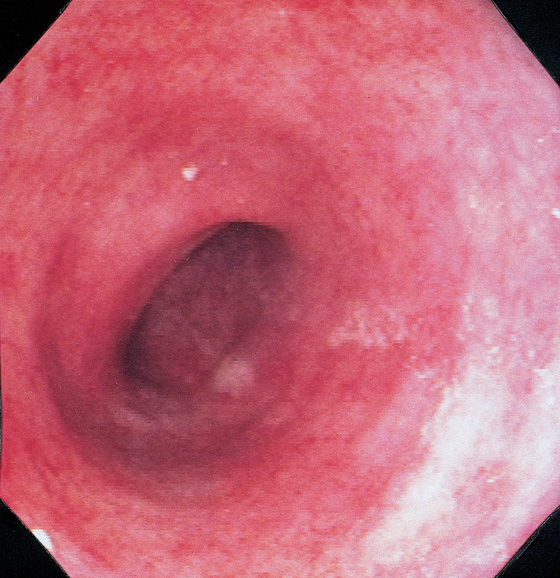
Figure 5.57 DIVERSION COLITIS
Hartmann’s pouch demonstrates loss of normal haustrations and vasculature, with diffuse subepithelial hemorrhage. Biopsy findings demonstrated normal architecture with edema, subepithelial hemorrhage, and mild chronic inflammatory infiltrate.
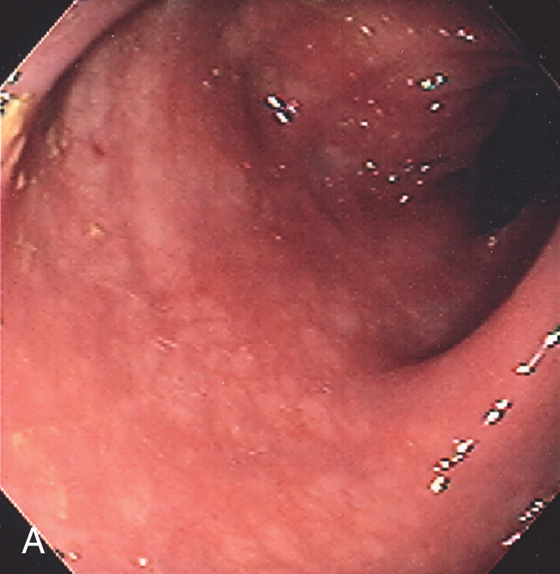
Figure 5.58 COLLAGENOUS COLITIS
A, Subtle loss of vascular pattern and erythema of the sigmoid colon. Typically, the colonic mucosa is normal.
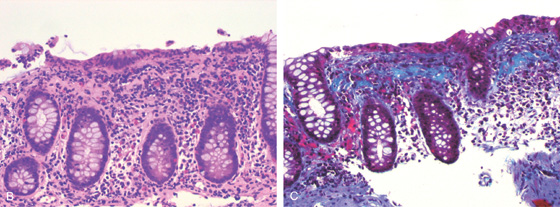
B, Hematoxylin and eosin stain suggests the diagnosis. C, Trichrome stain highlights the collagen layer in the subepithelium.
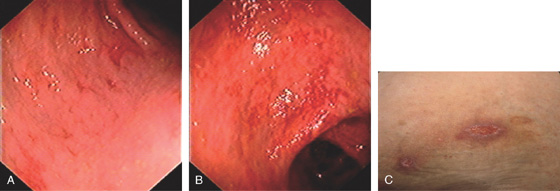
Figure 5.59 BEHÇET’S DISEASE
A, Edema with shallow ulcers in the distal colon. B, More extensive disease in the right colon with prominent subepithelial hemorrhage. C, Ulcer of the skin.
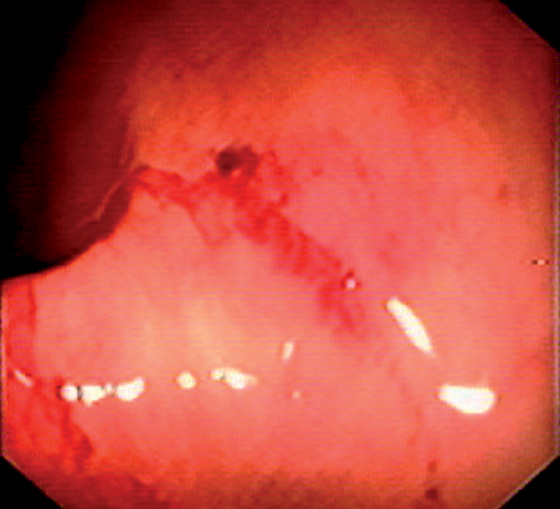
Figure 5.60 HENOCH-SCHÖNLEIN PURPURA
Subepithelial hemorrhage and recent bleeding.
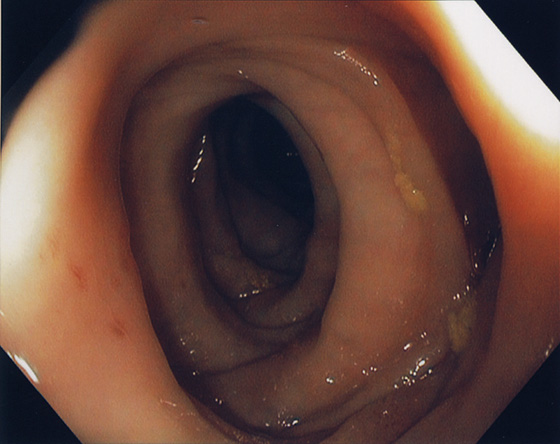
Figure 5.61 MUSCULATURE HYPERTROPHY ANTEDATING DIVERTICULOSIS
Circumferential thickening of musculature antedating diverticula formation.
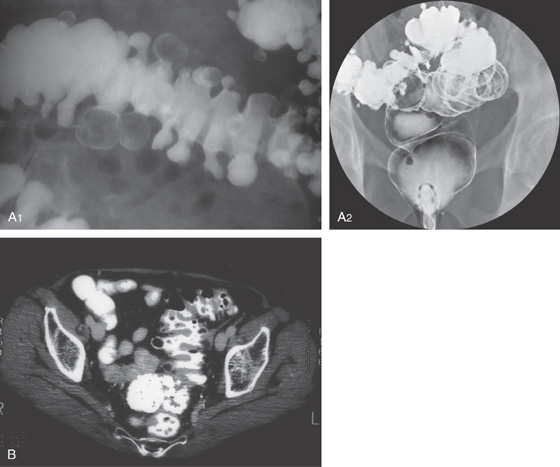
Figure 5.62 DIVERTICULOSIS
A1, Large diverticula filled with stool. The haustra are thickened. A2, Barium enema demonstrated sigmoid diverticulosis. B, Multiple diverticula in the sigmoid colon with thickened haustra.
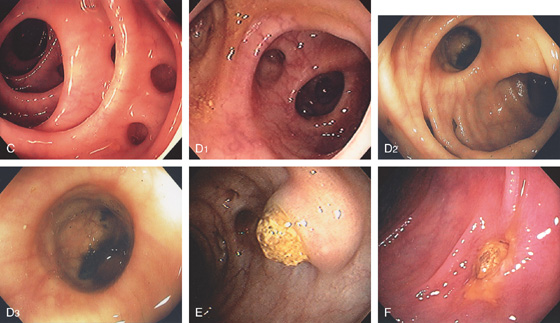
Figure 5.62 DIVERTICULOSIS
C,
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


