Chapter 4 Chronic viral hepatitis
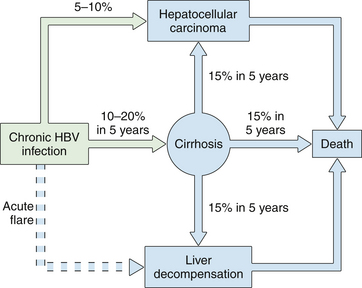
2 Long-term complications of chronic hepatitis include cirrhosis, liver failure, portal hypertension, and hepatocellular carcinoma.
3 Until recently, peginterferon plus ribavirin was the only approved treatment for chronic hepatitis C; overall more than 50% of patients treated with this dual therapy did not achieve viral eradication.
4 The direct-acting antiviral agents boceprevir and telaprevir were approved in May 2011 by the US Food and Drug Administration for the treatment of chronic hepatitis C genotype 1 infection in combination with peginterferon and ribavirin; the sustained virologic reponse rates up to 66% and 79%, respectively, with the addition of one of these two protease inhibitors to peginterferon plus ribavirin. In addition, approximately half to two-thirds of patients can achieve these high rates of viral eradication with only 24 to 28 weeks of therapy.
5 Seven drugs are approved for the treatment of chronic hepatitis B: interferon and peginterferon, three nucleoside analogues (lamivudine, telbivudine, entecavir), and two nucleotide analogues (adefovir and tenofovir); entecavir and tenofovir are the current first-line agents.
6 Hepatitis B virus mutates in response to antiviral drug treatment, which may lead to drug resistance, cross-drug resistance, and multidrug resistance; long-term treatment is required in these patients.
Overview
1. Chronic hepatitis is a condition characterized by persistent liver inflammation for more than 6 months after initial exposure or diagnosis of liver disease.
2. Causes of chronic viral hepatitis are hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D virus (HDV), and, in some circumstances, hepatitis E virus (HEV).
Chronic Hepatitis B
Clinical features and natural history
1. Symptoms of chronic hepatitis range from none, to nonspecific complaints (fatigue, right upper quadrant pain), to complications of cirrhosis.
2. Extrahepatic manifestations occur in up to 20% of patients with chronic hepatitis B and include arthralgias, polyarteritis nodosa, glomerulonephritis, mixed essential cryoglobulinemia, and a few other rare syndromes.
3. The risk of chronicity depends on the age and immune function when a person is infected; chronic infection occurs in




4. Approximately 25% of adults who become chronically infected during childhood will die at some point in their lifetime of HBV-related liver cancer or cirrhosis.
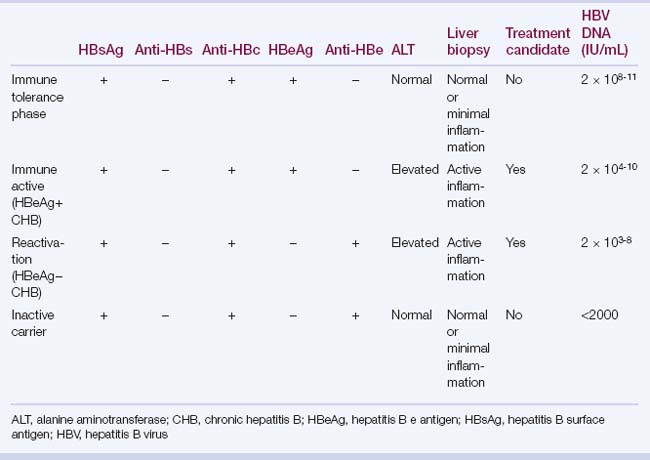
6. The prevalence of hepatitis B e antigen (HBeAg) declines with age, with spontaneous loss of HBeAg in 7% to 20% of patients per year.
7. Spontaneous loss of hepatitis B surface antigen (HBsAg) occurs infrequently (0.5% to 1% per year); with most patients developing anti-HBs.

Serologic and virologic tests (see Chapter 3)





Pathology and pathogenesis
1. HBV is a hepatotropic virus; most liver damage from HBV is caused by host immune responses with a cell-mediated response directed against cellular hepatitis B core antigen (HBcAg).
3. Non–antigen-specific immune responses, such as those mediated by inflammatory cytokines (tumor necrosis factor alpha, gamma interferon), may be more important for viral clearance than CTL-mediated mechanisms.
4. A hyperactive host response may lead to fulminant hepatitis, whereas a reduced host response increases the risk of chronic infection.
6. Nonspecific histologic findings include a predominantly lymphocytic infiltrate, which may or may not be confined to the portal tracts.
7. Characteristic histologic findings of chronic hepatitis B: these include ground-glass hepatocytes in which the cytoplasm is stained pink with hematoxylin-eosin in response to massive production of HBsAg; HBcAg can be demonstrated in the hepatocyte nuclei, within the cytoplasm and on the cell membrane.
Treatment
1. Goals of treatment
 Prevention of long-term complications (cirrhosis, hepatocellular carcinoma) and mortality by durable suppression of serum HBV DNA
Prevention of long-term complications (cirrhosis, hepatocellular carcinoma) and mortality by durable suppression of serum HBV DNA
Prevention of long-term complications (cirrhosis, hepatocellular carcinoma) and mortality by durable suppression of serum HBV DNA

4. Drugs



d. Rates of HBeAg seroconversion, undetectable HBV DNA, and normal ALT at 1 year of therapy are shown in Table 4.4.











5. Duration of HBV therapy with nucleos(t)ide analogues
 HBeAg positive: treat until HBeAg seroconversion, and stop after consolidation period 6 to 12 months after HBeAg seroconversion.
HBeAg positive: treat until HBeAg seroconversion, and stop after consolidation period 6 to 12 months after HBeAg seroconversion.
HBeAg positive: treat until HBeAg seroconversion, and stop after consolidation period 6 to 12 months after HBeAg seroconversion.
6. Resistance to antiviral drugs








d. Management of resistance (Table 4.6); roadmap for management of patients receiving oral antivirals for chronic hepatitis B (Fig. 4.2)
TABLE 4.3 Indications for HBV treatment
| Evidence of benefit: treatment indicated | Treatment not indicated |
|---|---|
| Decompensated cirrhotic patients | Immune tolerance phase |
| HBV DNA–positive cirrhotic patient | Inactive chronic carrier |
| Fulminant liver failure | Acute hepatitis B |
| HBsAg-positive patient who is going to be immunosuppressed | |
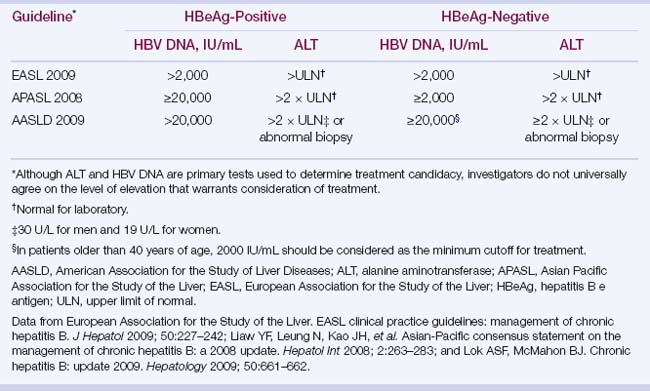
| Chronic hepatitis B with elevated ALT levels and HBV DNA >2000 UI/mL |
ALT, alanine aminotransferase; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus.
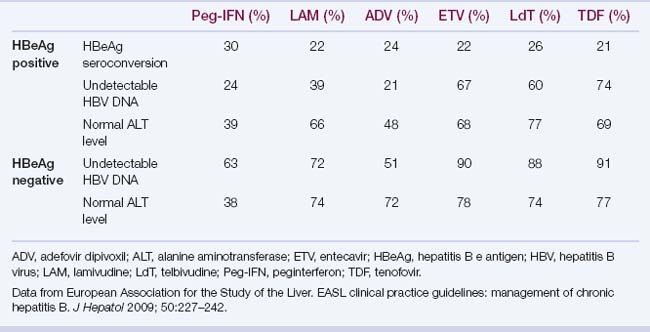
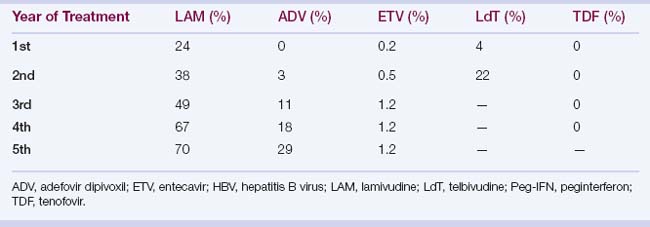
TABLE 4.6 Management of resistance to HBV antiviral drugs
| Resistance | Rescue Therapy |
|---|---|
| Lamivudine |




