and Armanda Tatsas2
(1)
Department of Pathology, The Johns Hopkins University School of Medicine, Baltimore, MD, USA
(2)
Pathology Group of Louisiana, Baton Rouge, LA, USA
Specimen Procurement and Preparation
Brush sampling of the bile ducts is performed either during endoscopic retrograde cholangiopancreatography (ERCP) or aspirated during percutaneous transhepatic cholangiography. Brushes can be directly smeared onto slides and stained using either Diff-Quik or Papanicolaou stain. They are either submitted intact submerged in ethanol-based solution, prepared by Cytospin method, and stained with Papanicolaou stain, or rinsed in a liquid-based cytology preservative solution and prepared using the liquid-based cytology platform methods. Some studies report improved detection of adenocarcinoma in bile duct brushings prepared using ThinPrep® technology over conventional smears due to better cellular preservation. There are no standardized criteria for adequacy in bile duct brushings or aspirations.
The reported sensitivity ranges from 30 to 88 % (mean 55 %). This relatively low sensitivity is attributed to either sampling error or interpretative error. Sampling error may be due to lesion size, location, extensive fibrosis, benign epithelium overlying a mass lesion, or technical difficulties, possibly related to experience of operator. Interpretative errors result from subtle changes in well-differentiated neoplasms which are difficult to definitively diagnose, or from lack of familiarity with the specimen type and poor cellular preservation. Sensitivity can be increased with repeat brushing. The overall reported specificity is 87–100 % (mean 97 %), thus the diagnosis is quite reliable if positive for malignancy.
Benign/Normal Biliary Epithelium
It is important to recognize the features of benign and reactive biliary epithelium in order to accurately diagnose adenocarcinoma in bile duct specimens. Benign biliary epithelium displays an orderly flat sheet of evenly spaced nuclei displaying a “honeycomb” arrangement. The nuclei are uniform in size, round to oval, with smooth nuclear contours and little to no nuclear overlap, and they are typically centrally placed in the cytoplasm of the cell. The nuclear to cytoplasmic ratio is low, though not as low as hepatocytes, as there is a moderate amount of finely granular cytoplasm, in contrast to the coarsely granular cytoplasm of hepatocytes. Small nucleoli are acceptable in benign epithelium (Figs. 4.1 and 4.2).
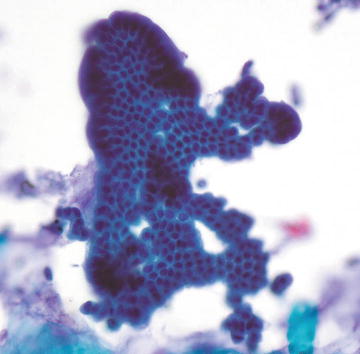
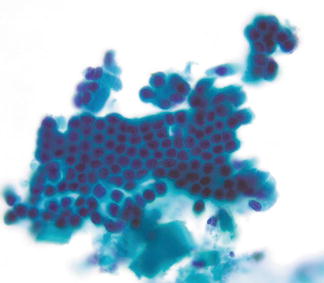
Fig. 4.1.
Biliary epithelium, normal: A fragment of normal, well-organized biliary epithelium is shown. The nuclei are small and evenly spaced in a honey comb arrangement with no overlap. (Biliary duct brush, Papanicolaou stain, medium power)
Fig. 4.2.
Biliary epithelium, normal: This fragment of biliary epithelium shows evenly sized, round nuclei which are centrally placed in a moderate amount of cytoplasm with ill-defined cell borders. The nuclei are uniformly spaced and show no overlap. (Biliary duct brush, Papanicolaou stain, medium power)
Key features:
Cohesive orderly monolayer sheets with a “honeycomb” arrangement
Evenly spaced, uniformly sized nuclei
Little to no nuclear overlap
Moderate amount of finely granular cytoplasm
Low n/c ratio
Round to oval nuclei with smooth nuclear contours
Occasional small nucleoli
Reactive Biliary Epithelium
Reactive epithelium may result from bouts of chronic pancreatitis, stones, or stent placement and can show focal marked atypia that may be mistaken for adenocarcinoma. Disruption of the normal “honeycomb” architecture occurs with unevenly spaced nuclei. Nuclei are often enlarged, typically in the range of two to three times normal size, and show small- to intermediate-sized nucleoli, sometimes multiple. Importantly, nuclear contours are smooth in contrast to the nuclear membrane irregularities seen in adenocarcinoma. The background in reactive processes often shows inflammatory cells, acute or chronic, and may show debris and bile pigment. If inflammatory cells are embedded in the ductal epithelium, a diagnosis of reactive atypia should be strongly considered prior to rendering a malignant diagnosis (Figs. 4.3, 4.4, 4.5, and 4.6).
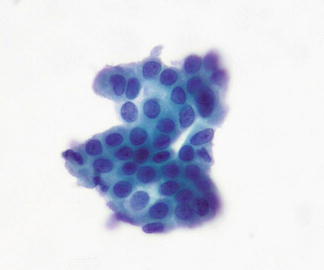
Fig. 4.3.




Biliary epithelium, reactive: This fragment of biliary epithelium shows very mild nuclear enlargement and slight disorganization of the honeycomb arrangement, though there is still no nuclear overlap. Nuclear contours are smooth and there are scattered small nucleoli. (Biliary duct brush, Papanicolaou stain, high power)
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
