CHAPTER 8 BENIGN BILIARY DISEASE AND ANASTOMOSIS
CHOLECYSTECTOMY
OPERATION
Anatomy
The normal location of the neck of the gallbladder and the cystic duct is between the peritoneal surfaces within the right anterior part of the hepatoduodenal ligament (Chapter 1). The cystic artery runs transversely, forming with the cystic duct and bile duct the triangle described by Calot (1891). The triangle of cholecystectomy (often misnamed as Calot’s triangle) has for its upper limit not the cystic artery but the inferior surface of the liver (Rocko et al., 1981). Dissection of this area should show the anatomic structures and allow safe dissection (Fig. 8-1).
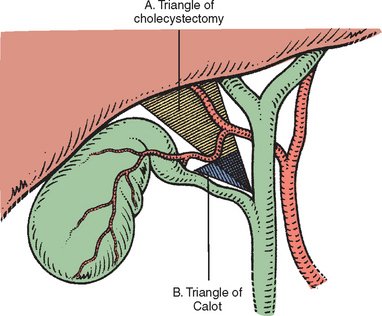
Several abnormalities can alter the normal anatomy of the gallbladder (Fig. 8-2). The junction between the cystic duct and the common bile duct (CBD) also has many variations (Figs. 8-3 and 8-4) and probably represents the most important source of error leading to damage of the biliary tract during cholecystectomy.

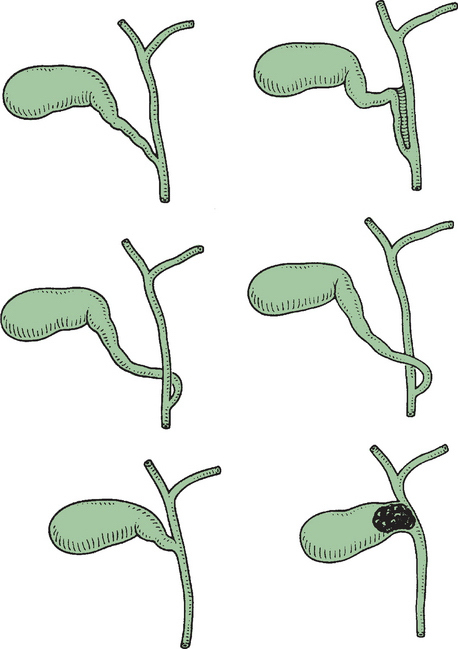
Figure 8-3 Different modes of confluence of the cystic duct and common hepatic duct (see also Chapter 1).
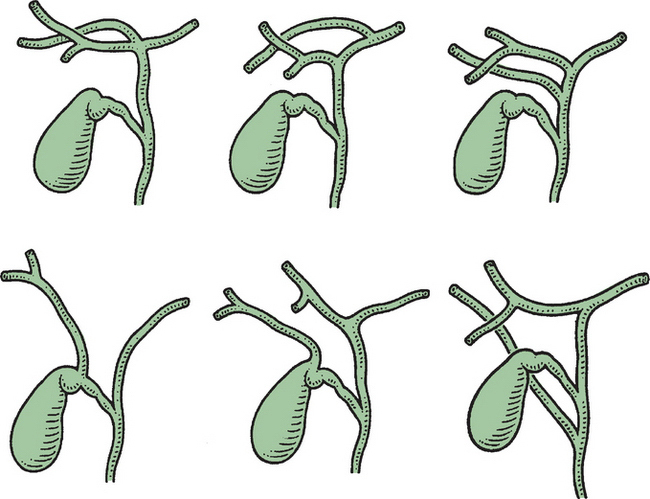
Figure 8-4 Variations in the confluence of the extrahepatic bile ducts and cystic duct (see also Chapter 1).
The right branch of the hepatic artery may be transected inadvertently if it is not identified. An origin of the right hepatic artery from the superior mesenteric artery results in passage of the vessel posterolaterally to the CBD and behind the cystic duct, where it may be vulnerable. Intraoperative cholangiography, besides showing unidentified stones or pathology in the intrahepatic or extrahepatic bile ducts, also provides a precise view of the anatomy of the biliary ductal system.
Retrograde Cholecystectomy
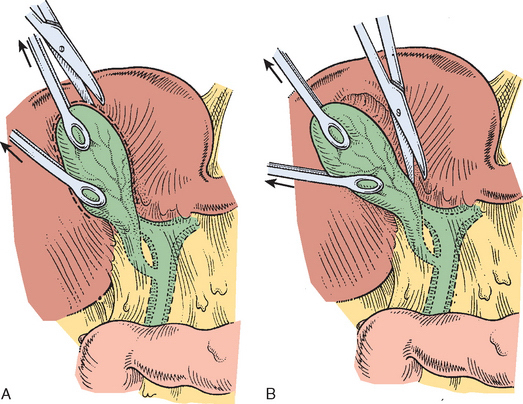
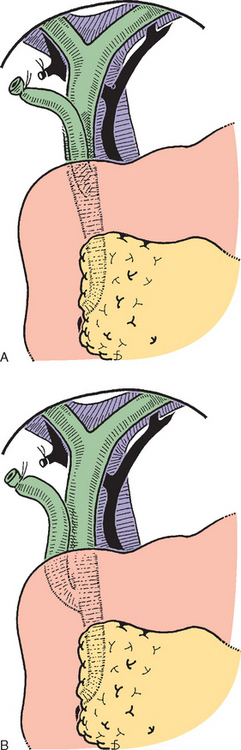
The peritoneum covering the hepatoduodenal ligament is incised. A clamp is placed at the fundus of the gallbladder, and the region of Hartmann’s pouch (Fig. 8-5) and of the cholecystectomy triangle is dissected. It is important to keep close contact with the gallbladder and to show the junction between the gallbladder and the cystic duct. A ligature is passed around the cystic duct but not tied. The cystic artery is dissected toward the gallbladder (see Fig. 8-5). The cystic duct is palpated to detect stones (Fig. 8-6). The cystic artery is ligated and transected (Fig. 8-7).
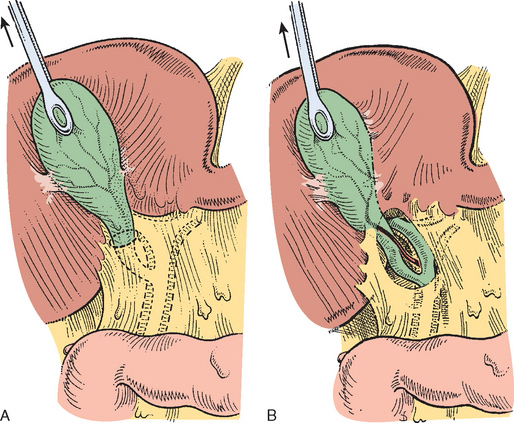
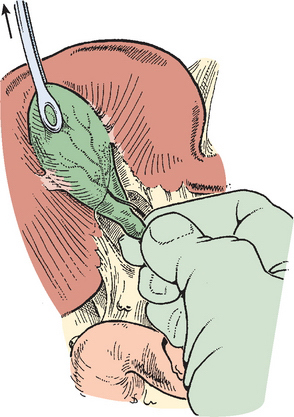
Figure 8-6 Palpation reveals a stone in the cystic duct, which may be “milked” back into the gallbladder.
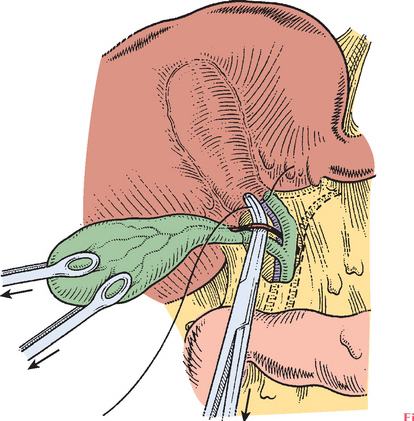
A ligature or a clamp is placed at the junction of the gallbladder, and a cannula for cholangiography is inserted into the cystic duct (Fig. 8-8). This catheter is fixed by tying the ligature previously passed around the cystic duct. Cholangiography is then performed. The cystic duct may then be divided. The gallbladder is then dissected from its fossa with the help of gentle traction. The dissection should be kept close to the gallbladder, within the cystic plate (see Chapter 1).
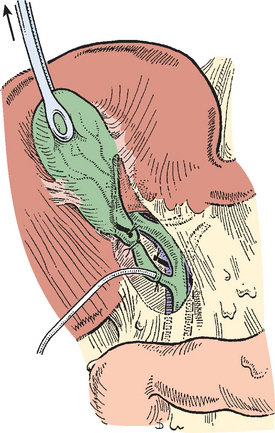
The cholangiography catheter is removed and the cystic duct is suture ligated using absorbable suture material (Fig. 8-9). Insertion of a drain is, in most cases, unnecessary.
Antegrade or Fundus-Down Cholecystectomy
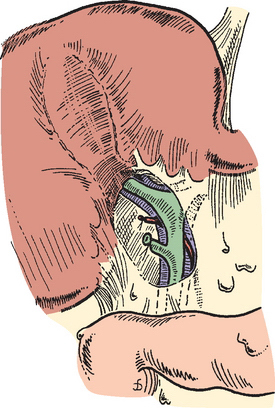
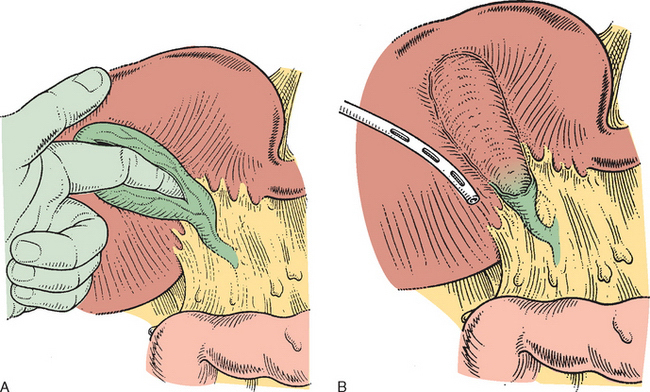
An incision of the gallbladder serosa overlying the fundus is performed, and a plane is developed by sharp dissection to allow entry to the cystic plate. The gallbladder is still vascularized via the cystic artery (Fig. 8-10). The cystic artery is encountered, seen to enter the gallbladder wall (Fig. 8-11), and divided. The infundibulum is dissected free down to the junction with the cystic duct. Cholangiography and cystic duct suture ligation are performed in the same way as described for the retrograde technique.
Partial Cholecystectomy
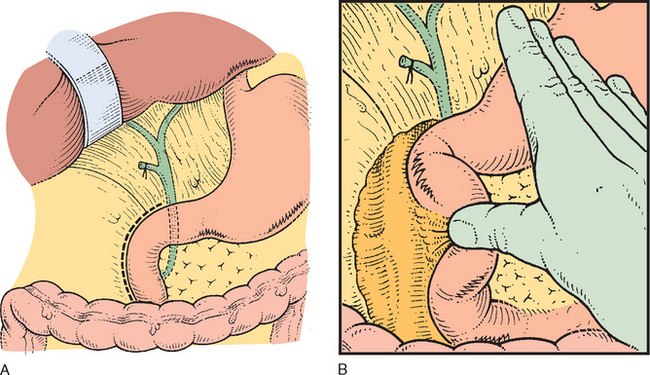
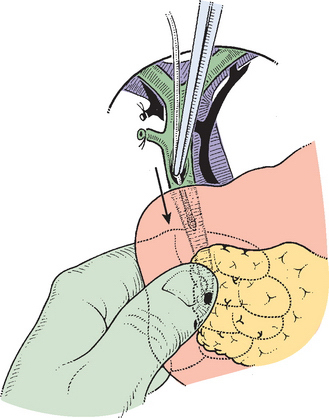
Cholecystectomy may be hazardous because fibrosis and inflammation obscure the triangle of Calot (Fig. 8-12). It is judicious to open the fundus and to introduce a finger into the gallbladder to guide the dissection (Fig. 8-13). Impacted stones should be removed.
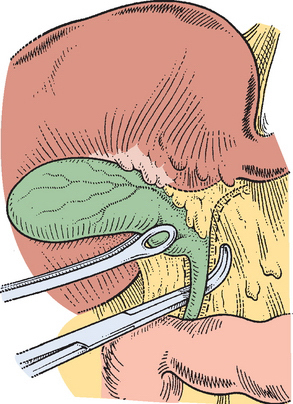
If no bile appears, the cystic duct is probably occluded by fibrosis and inflammation. A partial cholecystectomy is the safest procedure in this situation (see Fig. 8-13). No attempt at defining and ligating the cystic duct should be made. If a gush of bile appears when a large impacted stone is removed from the infundibulum, a cholecystocholedochal fistula is probably present (Mirizzi syndrome type II). It is advisable to keep the opened distal part of the gallbladder intact to allow performance of a cholecystoduodenostomy or a cholecystojejunostomy. Attempted direct repair of the fistula is unnecessary, difficult, and potentially hazardous (Baer et al., 1990).
INTRAOPERATIVE PROBLEMS
Dangerous surgery arises from inadequate or imprecise observation of the technical principles of cholecystectomy, insufficient experience, inadequate incision and exposure, or inadequate assistance. Some of the anatomic variations that have been mentioned previously (see Figs. 8-3 and 8-4, Chapter 1) are particularly dangerous.
Dangerous pathology includes chronic or acute inflammation, which results in obscured anatomy and increased vascularity in the region of the cholecystectomy triangle (see Fig. 8-12). Portal hypertension is associated with increased venous collateralization, which makes the dissection hemorrhagic and dangerous. Partial cholecystectomy is advocated in both situations.
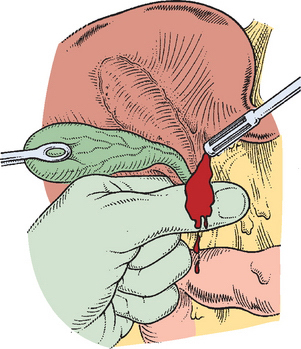
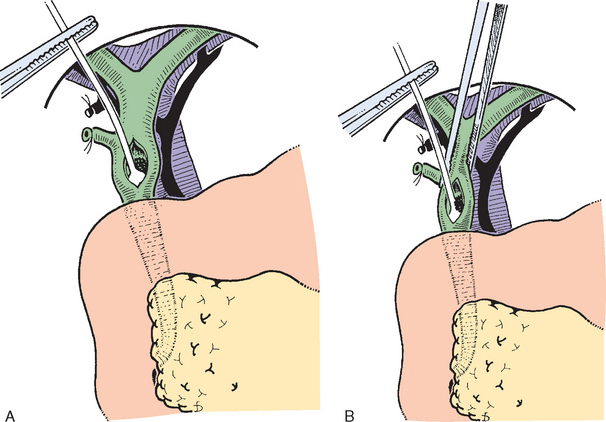
Hemorrhage in the cholecystectomy triangle represents potential danger because attempts at hemostasis by placing clamps with obstructed and insufficient view may result in inadvertent clamping of the right or proper hepatic artery or of the bile duct (Fig. 8-14). In this situation one should first attempt to control the hemorrhage by digital compression or by clamping the hepatoduodenal ligament (Fig. 8-15) to localize its precise origin. Grasping the bleeding vessel should be done with precision so as to limit the risks of including another structure in the ligature.
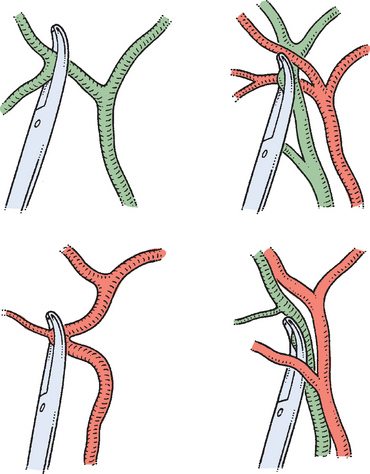
Figure 8-14 Blind placement of clamps for hemostasis can result in lesions of the hepatic artery or bile duct.
EXPLORATION OF THE COMMON BILE DUCT AND CHOLEDOCHOSCOPY
INDICATIONS FOR COMMON BILE DUCT EXPLORATION
The purpose of CBD exploration for choledocholithiasis is to detect and remove all stones within the bile duct system. The absolute indications for CBD exploration are (1) palpable stones in the CBD, (2) jaundice with cholangitis, and (3) a stone seen at intraoperative cholangiography (Fig. 8-16). Even where local endoscopic, radiologic, or laparoscopic expertise coexists, there are still indications for open choledochotomy:

SURGICAL TECHNIQUES FOR EXPLORATION OF THE COMMON BILE DUCT
Supraduodenal Choledochotomy and Exploration of the Common Bile Duct
Exposure
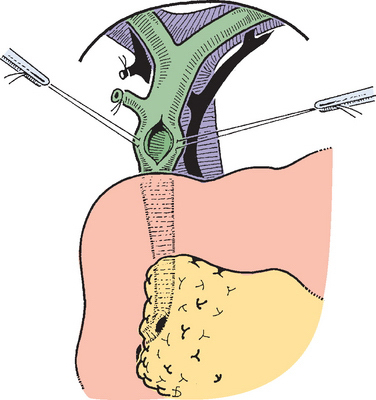
The liver is retracted superiorly and the hepatic flexure of the colon superiorly. The lesser omentum and stomach are retracted to the left. A Kocher maneuver is performed (Fig. 8-17).
Technique
The opening should be in the lowest part of the supraduodenal CBD (Fig. 8-18). A cystic duct lying anterior or closely applied to the CBD can be easily opened in error (Fig. 8-19). Bile is aspirated and sent for culture.
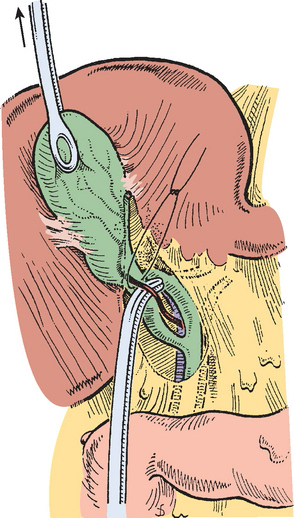
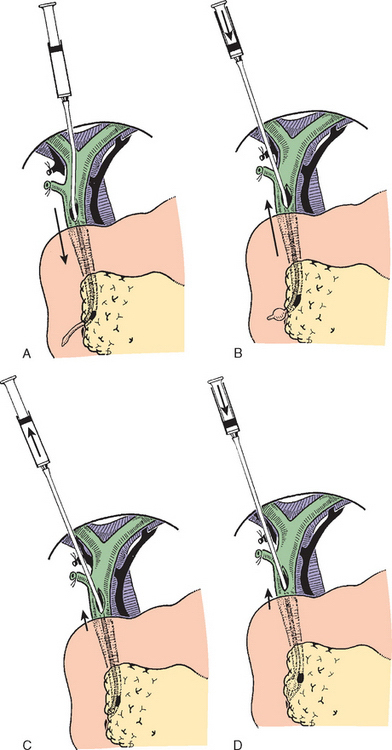
A Fogarty balloon catheter (Fogarty et al., 1968) is introduced into the CBD (Fig. 8-20) and passed into the duodenum (Fig. 8-21). The balloon is inflated, and the catheter is withdrawn until it impinges against the papilla. The second part of the duodenum and posterior surface of the head of the pancreas are palpated, and the balloon is identified. Any stone present usually can be felt against the shaft of the catheter. The balloon is deflated and gently withdrawn through the papilla; this is detected by a sudden easing of the pull on the catheter. The balloon is reinflated immediately (Fig. 8-21). The catheter is held by the syringe in the left hand; with gentle traction superiorly by forceps held in the surgeon’s right hand, the catheter is gradually pulled up to the choledochotomy site (Fig. 8-22), taking care to prevent any stone from slipping into the proximal biliary tree.
Postexploratory Investigations
T-Tube Cholangiography
After insertion of a T-tube and closure of the choledochotomy, T-tube cholangiography may be used for postexploratory investigation (Fig. 8-23).










