Fig. 10.1
Conventional view: a flat elevated lesion was seen on the anastomotic site in the transverse colon
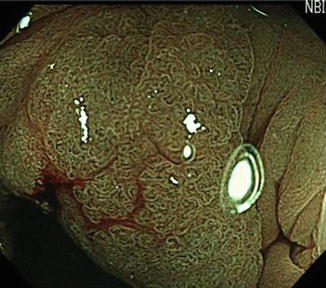
Fig. 10.2
NBI with magnifying colonoscopy revealed slightly dilated capillary vessels (type IIIA in Sano’s classification of capillary pattern)
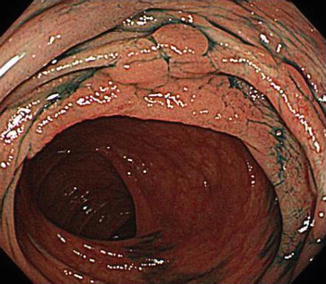
Fig. 10.3
Chromoendoscopy using indigo carmine dye spraying. The outline of the tumor was accentuated
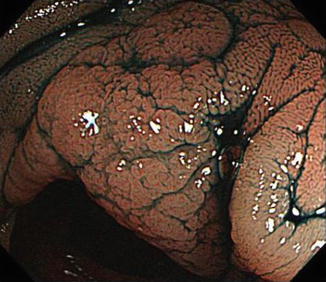
Fig. 10.4
Chromoendoscopy with magnification. Pits were irregular in shape, size, and arrangement (VI noninvasive pattern)

Fig. 10.5
Endoscopic submucosal dissection (ESD)
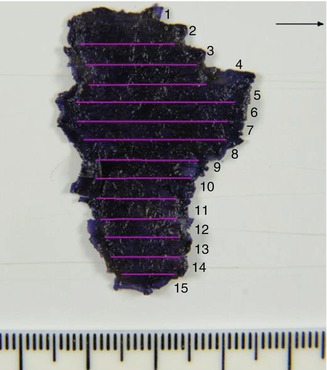
Fig. 10.6
Mapping of the resected specimen. The area showed by pink color lines revealed intramucosal cancer
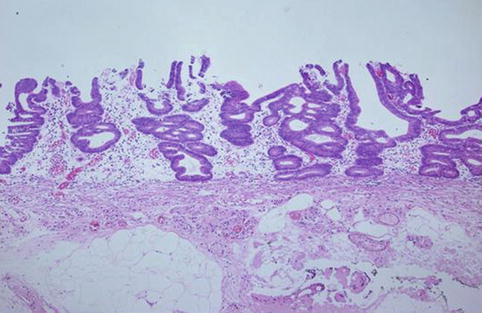
Fig. 10.7
Tubular adenocarcinoma, well differentiated
In this case, the previous doctor could not perform total colonoscopy before surgery due to severe stenosis. The lesion on the anastomotic site therefore should be a synchronous lesion. Surveillance colonoscopy should be performed with special attention to synchronous and metachronous colorectal cancers after this kind of surgery.
References
1.
2.
Fujii T, Hasegawa RT, Saitoh Y et al (2001) Chromoscopy during colonoscopy. Endoscopy 33:1036–1041PubMed
3.
Matsuda T, Fujii T, Saito Y et al (2008) Efficacy of the invasive/non-invasive pattern by magnifying chromoendoscopy to estimate the depth of invasion of early colorectal neoplasms. Am J Gastroenterol 103:2700–2706PubMedCrossRef
Related posts:
 Impact of Flexible Endoscopy in the Evaluation of Digestive Anastomosis
Impact of Flexible Endoscopy in the Evaluation of Digestive Anastomosis
 Therapeutic Endoscopy for the Treatment of Benign Anastomotic Strictures
Therapeutic Endoscopy for the Treatment of Benign Anastomotic Strictures
 Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Small Bowel Surgery
Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Small Bowel Surgery
 Review: Therapeutic Endoscopy for the Treatment of Anastomotic Dehiscences
Review: Therapeutic Endoscopy for the Treatment of Anastomotic Dehiscences
 Contribution of Endo-ultrasonography
Contribution of Endo-ultrasonography
 Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Esophageal Surgery
Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Esophageal Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


