, Adele Taibbi1 and Massimo Midiri1
(1)
Department of Radiology, University Hospital, Palermo, Italy
During the last decades, invasive and semi-invasive locoregional treatments have been developed and improved for the treatment of primary and secondary hepatic tumors. Efficacy of these therapies is usually monitored by means of contrast-enhanced CT and MR. The goal is documenting the lack of vascularization in the treated area and early detection of tumor recurrence allowing further treatments and thus increasing life expectancy.
CT and MR represent the gold standard for the evaluation of the therapeutic response after local treatments. But, as already confirmed by several studies, CEUS represents a reliable alternative technique since it allows the study in real time of microcirculation useful for an early detection of viable tissue [1]. Moreover, it represents a useful tool before locoregional treatments in order to better define lesion’s margins and for an adequate radiofrequency needle placement [2].
Also at CEUS, a complete response is considered achieved when there is no enhancing portion within or at the periphery of the treated area during the hepatic arterial phase [3, 4]. Residual unablated tumor is defined as a portion of treated HCC showing persistent hypervascularity in the arterial phase, usually appearing as an irregular peripheral-enhancing focus in the treated zone. When viable tumoral tissue, enhancing at arterial phase acquisition, is detected within the edge of a treated nodule, the pattern is called “in-growth” whereas when it is depicted around a necrotic treated nodule and in continuity with its border, the term “out-growth” could be used.
Immediately and up to 3 months after the treatment, a quite uniform and relatively thin (usually 4–5 to 7–8 mm thick) peripheral rim of contrast enhancement surrounding the treated zone can be evident as a local response to thermal damage due to benign reactive hyperemia [5]. The rim of hyperemia may sometimes be difficult to differentiate from actual residual tumor, but usually it is thin, completely surrounding the treated area, and disappears over time. Another area presenting as transient hypervascular area in the arterial phase may be related to the presence of arteriovenous shunting and may also lead to misinterpretation. This perfusion alteration becomes isoechoic to the surrounding liver parenchyma in the extended portal venous phase and the characteristics of a peripheral-based wedge-shaped pattern are helpful to differentiate this entity from residual tumor. The term tumor progression usually refers to the presence of growing enhancing tumors at the periphery of treated area at CEUS later than 1-month follow-up but with no evidence of residual tumor in the previous controls [6, 7].
6.1 Locoregional Treatment
6.1.1 RFTA
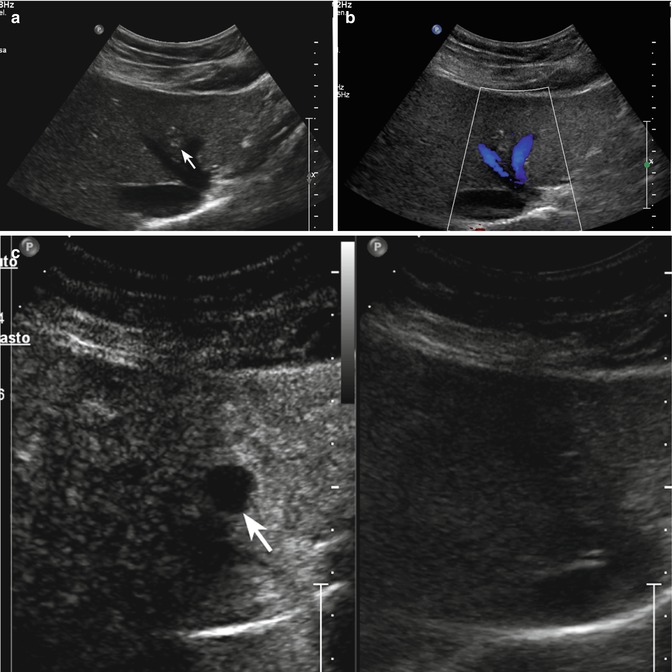
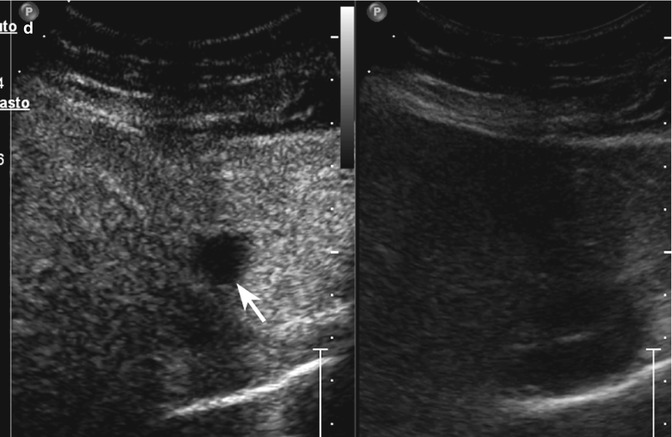
Fig. 6.1
Complete response in RFTA-treated colorectal metastasis in a 55-year-old woman. (a) Central subcostal baseline US image shows a 1 cm-sized slightly inhomogeneous hyperechoic area in the IV hepatic segment (arrow) without vascularization at color-Doppler evaluation (b). At CEUS, the lesion shows lack of contrast enhancement in the arterial (c) and extended portal-venous (d) phases (left, arrows)
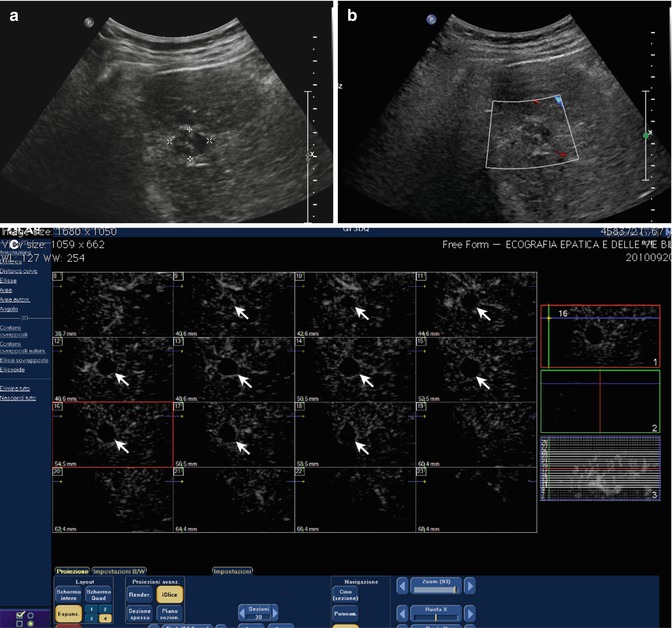
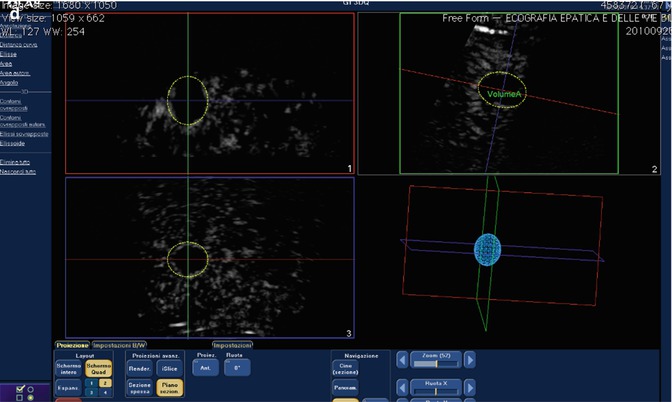
Fig. 6.2
Complete response after RFTA in a 49-year-old man. (a) Oblique ascending right subcostal baseline US image shows a 1.7 cm-sized inhomogeneous hypoechoic area in the V hepatic segment (calipers) without vascularization at color-Doppler evaluation (b); (c) At 3D-CEUS, i-Slice reconstruction shows lack of contrast enhancement in each slice during the arterial phase (arrows); (d) Volumetric reconstruction on three planes shows the entire volume of the treated area
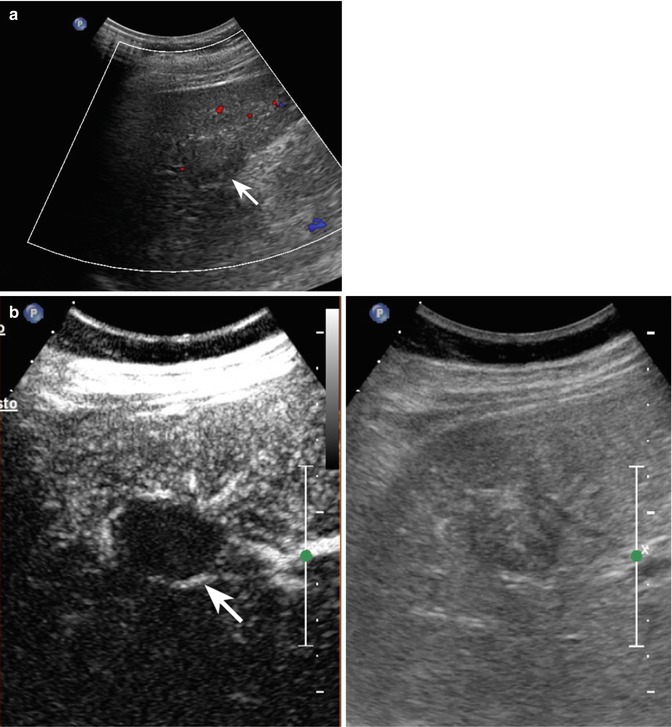
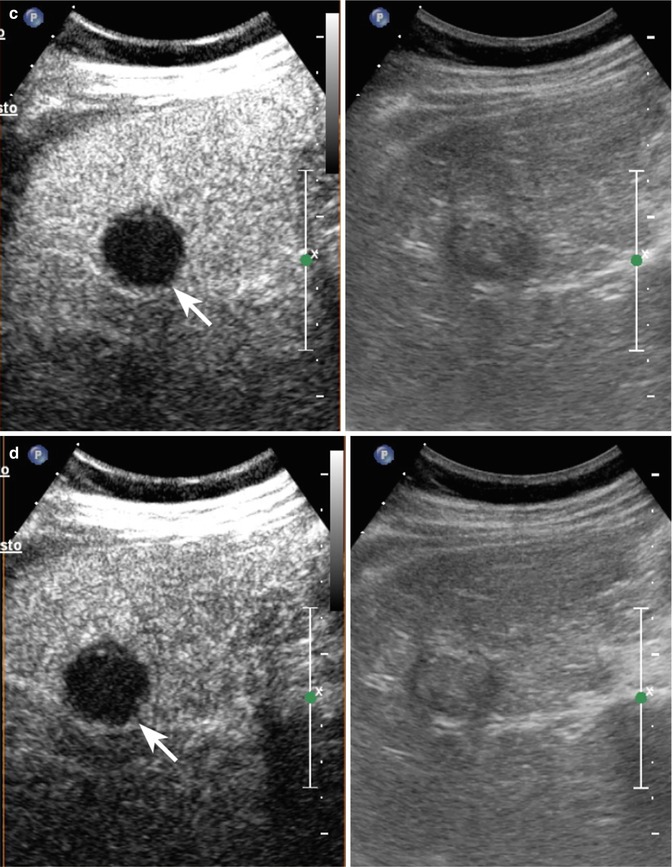
Fig. 6.3




Rim of hyperemia in RFTA-treated HCC in a 63-year-old man. (a) Oblique ascending right subcostal image reveals a slightly hypoechoic 3 cm-sized area in the V hepatic segment in the subcapsular region, with absence of vascularization at color-Doppler evaluation (arrow). (b) At CEUS 1 month after RFA, a thin peripheral rim of contrast enhancement surrounding the ablated zone is evident in the arterial phase (27 s after SonoVue injection) (left, arrow) and no more appreciable in the remaining portal-venous (c) and late phases (d) (arrows)
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
