Chapter 1 Assessment of liver function and diagnostic studies
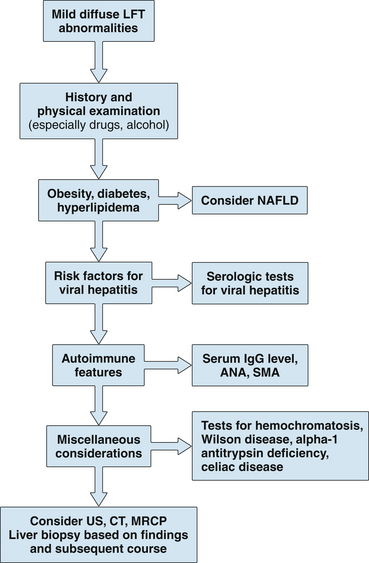
1 Reflecting the liver’s diverse functions, the colloquial term liver function tests (LFTs) includes true tests of hepatic synthetic function (e.g., serum albumin), tests of excretory function (e.g., serum bilirubin), and tests that reflect hepatic necroinflammatory activity (e.g., serum aminotransferases) or cholestasis (e.g., alkaline phosphatase).
2 Abnormal liver biochemistry test results are often the first clues to liver disease. The widespread inclusion of these tests in routine blood chemistry panels uncovers many patients with unrecognized hepatic dysfunction.
3 Normal or minimally abnormal liver biochemical test levels do not preclude significant liver disease, even cirrhosis.
4 Laboratory testing can assess the severity of liver disease and its prognosis; sequential testing may allow assessment of the effectiveness of therapy.
5 Liver biopsy remains the gold standard for assessing the severity of liver disease, as well as for confirming the diagnosis for some causes. Newer diagnostic noninvasive modalities including serum markers of fibrosis and transient elastography may complement the use of liver biopsy.
Routine Liver Biochemical Tests
Serum bilirubin


2. Metabolism
 Bilirubin is a breakdown product of hemoglobin and, to a lesser extent, heme-containing enzymes; 95% of bilirubin is derived from senescent red blood cells.
Bilirubin is a breakdown product of hemoglobin and, to a lesser extent, heme-containing enzymes; 95% of bilirubin is derived from senescent red blood cells.
 Bilirubin is released into blood and tightly bound to albumin; free or unconjugated bilirubin is lipid soluble, is not filtered by the glomerulus, and does not appear in urine.
Bilirubin is released into blood and tightly bound to albumin; free or unconjugated bilirubin is lipid soluble, is not filtered by the glomerulus, and does not appear in urine.
Bilirubin is a breakdown product of hemoglobin and, to a lesser extent, heme-containing enzymes; 95% of bilirubin is derived from senescent red blood cells. Bilirubin is released into blood and tightly bound to albumin; free or unconjugated bilirubin is lipid soluble, is not filtered by the glomerulus, and does not appear in urine.
Bilirubin is released into blood and tightly bound to albumin; free or unconjugated bilirubin is lipid soluble, is not filtered by the glomerulus, and does not appear in urine.





3. Measurement of serum bilirubin
a. van den Bergh reaction
 Total serum bilirubin represents all bilirubin that reacts within 30 minutes in the presence of alcohol (an accelerating agent).
Total serum bilirubin represents all bilirubin that reacts within 30 minutes in the presence of alcohol (an accelerating agent).
Total serum bilirubin represents all bilirubin that reacts within 30 minutes in the presence of alcohol (an accelerating agent).

4. Classification of hyperbilirubinemia
a. Unconjugated (bilirubin nearly always less than 7 mg/dL)
 Overproduction (presentation to liver of bilirubin load that exceeds hepatic capacity for uptake and conjugation): hemolysis, ineffective erythropoiesis, resorption of hematoma
Overproduction (presentation to liver of bilirubin load that exceeds hepatic capacity for uptake and conjugation): hemolysis, ineffective erythropoiesis, resorption of hematoma
Overproduction (presentation to liver of bilirubin load that exceeds hepatic capacity for uptake and conjugation): hemolysis, ineffective erythropoiesis, resorption of hematoma








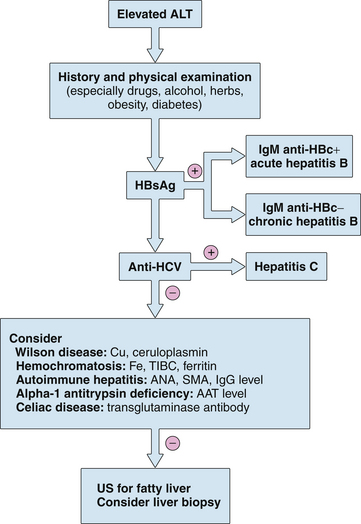
Serum aminotransferases (Table 1.1)
1. These intracellular enzymes are released from injured hepatocytes and are the most useful marker of hepatic injury (inflammation or cell necrosis).












5. Abnormally low aminotransferase levels have been associated with uremia and chronic hemodialysis; chronic viral hepatitis in this population may not result in aminotransferase elevation.
TABLE 1.1 Causes of elevated serum aminotransferase levels∗
| Mild elevation (<5× normal) | Marked elevation (>15× normal) |
|---|---|
| Hepatic: ALT predominant | Acute viral hepatitis (A–E, herpes) |
| Chronic viral hepatitis | DILI |
| Acute viral hepatitis (A–E, EBV, CMV) | Ischemic hepatitis |
| NAFLD | Autoimmune hepatitis |
| Hemochromatosis | Wilson disease |
| DILI | Acute bile duct obstruction |
| Autoimmune hepatitis | Acute Budd–Chiari syndrome |
| Alpha-1 antitrypsin deficiency | Hepatic artery ligation |
| Wilson disease | |
| Celiac disease | |
| Hepatic: AST predominant | |
| Alcohol-related liver injury (AST:ALT >2:1) | |
| Cirrhosis | |
| Nonhepatic | |
| Strenuous exercise | |
| Hemolysis | |
| Myopathy | |
| Thyroid disease | |
| Macro-AST |
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CMV, cytomegalovirus; DILI, drug-induced liver injury; EBV, Epstein-Barr virus; NAFLD, nonalcoholic fatty liver disease.
∗ Almost any liver disease may be associated with ALT levels 5 times to 15 times normal.
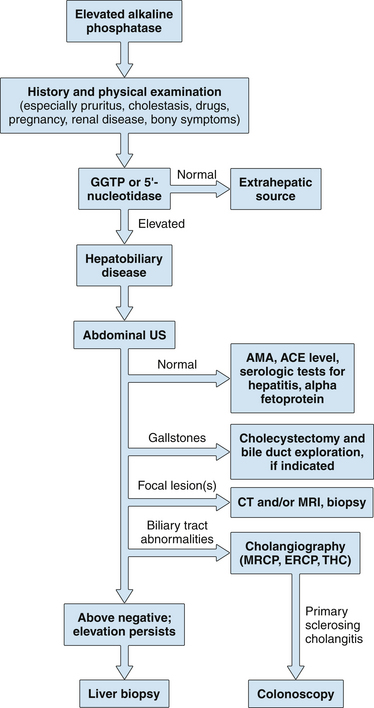
Serum alkaline phosphatase
1. Hepatic alkaline phosphatase is one of several alkaline phosphatase isoenzymes found in humans and is bound to hepatic canalicular membrane; various laboratory methods are available for its measurement, and thus comparison of results obtained by different techniques may be misleading.
2. This test is sensitive for detection of biliary tract obstruction (a normal value is highly unusual in significant biliary obstruction); interference with bile flow may be intrahepatic or extrahepatic.
 An increase in serum alkaline phosphatase results from increased hepatic synthesis of the enzyme, rather than leakage from bile duct cells or failure to clear circulating alkaline phosphatase; because it is synthesized in response to biliary obstruction, the alkaline phosphatase level may be normal early in the course of acute suppurative cholangitis when the serum aminotransferases are already elevated.
An increase in serum alkaline phosphatase results from increased hepatic synthesis of the enzyme, rather than leakage from bile duct cells or failure to clear circulating alkaline phosphatase; because it is synthesized in response to biliary obstruction, the alkaline phosphatase level may be normal early in the course of acute suppurative cholangitis when the serum aminotransferases are already elevated.
An increase in serum alkaline phosphatase results from increased hepatic synthesis of the enzyme, rather than leakage from bile duct cells or failure to clear circulating alkaline phosphatase; because it is synthesized in response to biliary obstruction, the alkaline phosphatase level may be normal early in the course of acute suppurative cholangitis when the serum aminotransferases are already elevated.

3. Isolated elevation of alkaline phosphatase
 Nonhepatic sources of alkaline phosphatase are bone, intestine, kidney, and placenta (different isoenzymes); striking elevations are seen in Paget’s disease of the bone, osteoblastic bone metastases, small bowel obstruction, and normal pregnancy.
Nonhepatic sources of alkaline phosphatase are bone, intestine, kidney, and placenta (different isoenzymes); striking elevations are seen in Paget’s disease of the bone, osteoblastic bone metastases, small bowel obstruction, and normal pregnancy.

 Nonhepatic sources of alkaline phosphatase are bone, intestine, kidney, and placenta (different isoenzymes); striking elevations are seen in Paget’s disease of the bone, osteoblastic bone metastases, small bowel obstruction, and normal pregnancy.
Nonhepatic sources of alkaline phosphatase are bone, intestine, kidney, and placenta (different isoenzymes); striking elevations are seen in Paget’s disease of the bone, osteoblastic bone metastases, small bowel obstruction, and normal pregnancy.


5. Low serum levels of alkaline phosphatase may occur in hypothyroidism, pernicious anemia, zinc deficiency, congenital hypophosphatasia, and fulminant Wilson disease.