and Christopher Isles2
(1)
Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, UK
(2)
Dumfries and Galloway Royal Infirmary, Dumfries, UK
Q1 How accurate is blood urea as a measure of renal function?
When we talk about “renal function” we usually mean the glomerular filtration rate (GFR). Each kidney has around 1,000,000 nephrons and the GFR is a measure of the function of all of these in both kidneys. Urea is a nitrogenous waste product, the level of which in the blood is usually <7 mmol/l. Blood urea rises in patients with kidney injury but is an imperfect marker of GFR for the following reasons: urea generation is low in patients with chronic liver disease and malnutrition and is disproportionately increased in those who are dehydrated (because urea is reabsorbed passively with sodium and water by the proximal tubule) or those who have gastrointestinal blood loss (because urea is absorbed from the gut).
Q2 How accurate is serum creatinine as a measure of renal function?
Still imperfect but better than urea. The normal range for serum creatinine is usually given as 60–125 umol/l though all this means is that 95 % of the adult population will have a serum creatinine that lies somewhere between these two levels – serum creatinine of 125 umol/l is actually quite abnormal (see below). Creatinine is derived from creatine which is a protein found in muscle. It follows that creatinine levels will be lower in the elderly because of their lower muscle mass and higher in weight lifters. The important consequence of low muscle mass in the elderly is that elderly patients may have quite advanced renal failure with only modest elevations of their serum creatinine
Q3 What is the relation between serum creatinine & glomerular filtration rate (GFR)?
A useful rule of thumb is that every time the creatinine doubles the GFR will halve. Thus, if serum creatinine of 62.5 μmol/l and a GFR of 100 ml/min is our starting point, this means that by the time serum creatinine has gone above the upper limit of the normal range (approximately 125 μmol/l), 50 % of glomerular function has already been lost; also that when serum creatinine exceeds 500 μmol/l the GFR will have fallen below 12.5 ml/min (Fig. 2.1).
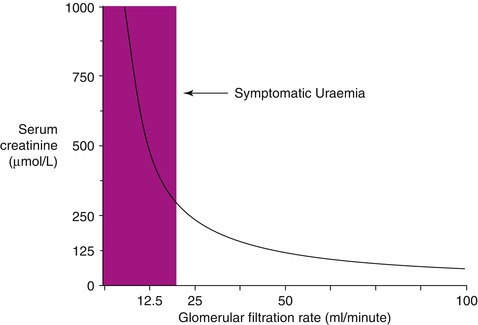
Fig. 2.1
Relationship of serum creatinine to GFR
Q4 How was GFR assessed in the past?
Previously we assessed GFR by collecting urine for 24 h and measuring creatinine clearance using the formula UV/P where U = urine creatinine in μmol/l, V = volume of urine passed in ml/min and P = serum creatinine in μmol/l. This method has fallen out of favour. Not only was the collection messy and cumbersome but patients often forgot to include all the urine they passed and sometimes failed to understand that the first specimen of urine on the first day had to be discarded (Fig. 2.2)
Fig. 2.2
Twenty four hour urine collection sample
Q5 How is GFR assessed now?
The standard method of estimating GFR now is based on the MDRD equation (so called because it was used in the study on the Modification of Diet and Renal Disease) which estimates GFR on the basis of a patient’s age, serum creatinine, gender and race. All biochemistry departments in the UK now use this formula to estimate GFR. If you want to calculate eGFR on an existing creatinine result there is an easy to use calculator on the website of the Renal Association at http://egfrcalc.renal.org/




Q6 What is the Cockcroft-Gault equation?< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
