(1)
Department of Vascular Surgery, Evangelisches Krankenhaus Königin Elisabeth Herzberge, Berlin, Germany
W.D. Brittinger had the basic idea for this kind of hemodialysis access. He was the first to publish the superficialization of the superficial femoral artery for puncture (Brittinger et al. 1969), which was abandoned because of frequent microembolisms. In 1994 the access described below was developed for a patient in whom all large deep veins were occluded.
Principle
Interposition of a prosthetic loop graft into the infraclavicular axillary artery or common femoral artery.
Indication
An arterioarterial graft for hemodialysis is only rarely indicated. There are four indications:
1.
All six large deep veins (femoral, jugular, and subclavian) are occluded or not suitable due to septic complications.
2.
Only one of the six large deep veins is patent, which has to be preserved as an emergency access.
3.
With heart failure refractory to therapy, the increased cardiac output induced by an AV access would impair the preexisting dysfunction even further.
4.
Peripheral vascular disease with inadequate limb perfusion:
Already without an AV access of the extremity and/or
After proximalization of the arterial inflow into an AV shunt from the feeding infraclavicular axillary artery
5.1 Physiology of Arterioarterial Grafts
To guarantee a sufficient flow for effective dialysis, the following requirements have to be fulfilled:
Always insert the loop graft into the course of the artery and not just as a bypass to a patent artery, for then the flow in the prosthetic graft would be relatively low due to the flow distribution. Dialysis could be ineffective with a high risk of thrombosis.
Only choose a large artery with a high flow volume. Thus only the infraclavicular axillary artery and the common femoral artery are practicable options.
Definite physiologic advantages of arterioarterial interpositon grafts include their lack of influence on:
Cardiac output
Peripheral perfusion
Take care to add only drugs to the dialysate which are approved for intraarterial administration.
Due to the flow rate (typically around 150–250 mL/min), which is significantly lower than in AV shunts, the time required for a dialysis session is longer (frequently 5–6 h). Large surface area dialyzers increase the efficiency of hemodialysis.
5.2 Infraclavicular Arterioarterial Graft
Indication
Preferred to femoral position.
Prerequisite
Patent arterial vasculature of the upper extremity.
Contraindication
Amputation of the ipsilateral arm (with low flow perfusion).
Approach
Exposure of the artery via an infraclavicular transverse incision and placement of the prosthetic graft into a looped subcutaneous tunnel of the ventral thoracic wall (Fig. 5.1)
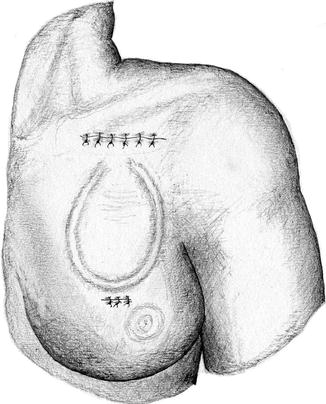
Fig. 5.1




Subclavian arterioarterial graft
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
