(1)
Department of Vascular Surgery, Evangelisches Krankenhaus Königin Elisabeth Herzberge, Berlin, Germany
With only 0.3 % of all AV access cases, arterial reconstructions related to AV accesses are rare events in our patients. Arterial stenoses and occlusions of the large vessels (subclavian, axillary, and femoral arteries) are almost exclusively caused by atherosclerotic changes, whereas in peripheral arteries secondary changes after AV surgery are predominant.
12.1 Clinical Presentation and Investigations
12.1.1 Reduced Arterial Inflow into the AV Access
A reduced thrill and a slowed refilling after emptying the vessel are signs of an arterial inflow that is too low (cf. Chap. 18). Then the pressure in the AV access is also reduced. During dialysis, pathologic recirculation may be present. There are different causes (Fig. 12.1):
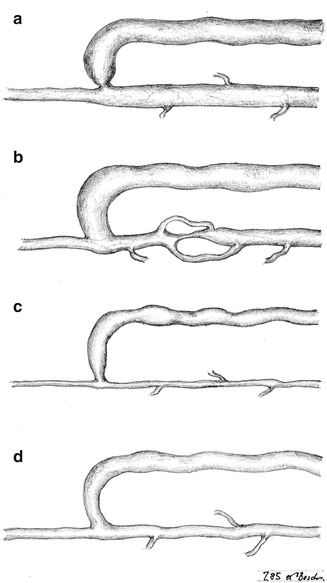
Fig. 12.1
Potential causes of a low arterial inflow. (a) Stenosis of the anastomosis. (b) Stenosis of the feeding artery. (c) Narrow artery. (d) Hypotension with sufficient artery
Often sonography is sufficient to find the correct diagnosis. If there is a suspicion or proof that the feeding artery is occluded, we also rely on arteriograms.
12.1.2 Insufficient Peripheral Perfusion
Mainly in patients with repeated previous AV access surgery or surgery dating back some time, multiple arterial occlusions or stenoses may lead to clinically relevant insufficient perfusion with symptoms ranging from pain to tissue loss (Chap. 11). Duplex sonography may prove helpful, but before surgery we also order arteriograms if indicated.
12.1.3 Indications for Arterial Reconstructions
An occlusion or stenosis should only be treated if it causes relevant symptoms or loss of function.
Indications for arterial reconstructions are:
Indadequately low arterial feeding of the AV access
Indadequately low peripheral perfusion
The following is based on our experience in 59 documented cases from 1982 through 2011.
12.2 Reconstruction of Upper Extremity Arteries
Taking into account anatomy, occurrence of stenoses, and therapy, we suggest dividing the arteries of the arm into seven (I–VII) segments (Fig. 12.2).
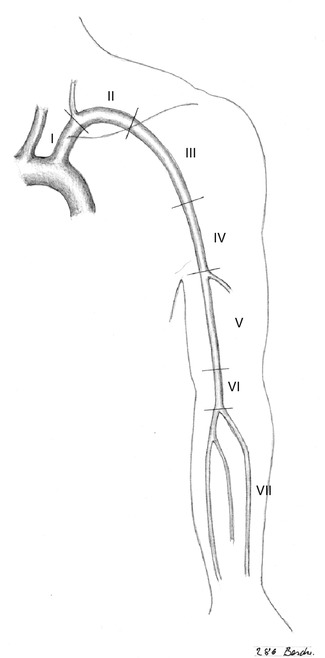
Fig. 12.2
Division of the arm arteries into seven segments according to surgical aspects
12.2.1 Segment I: Stenoses/Occlusions of the Central Subclavian Artery (Aortovertebral Segment) (n = 5)
If the vertebral artery is patent, a steal effect may arise. In general, endovascular treatment should be tried first, which is successful in about 75 % of these cases. Only if it fails will surgery be indicated. There are three local options. Vascular morphology and topography dictate the choice.
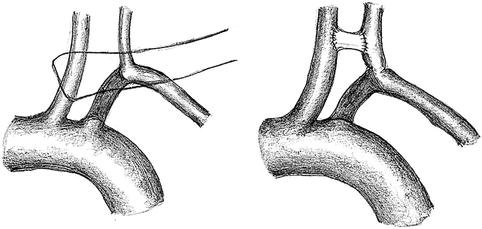
Transposition of the Subclavian to the Common Carotid Artery (Fig. 12.3)
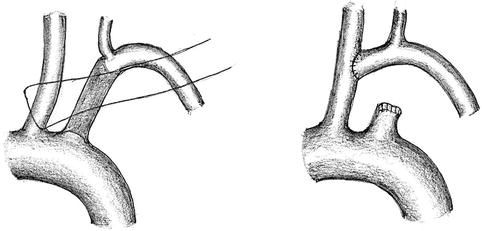
Fig. 12.3
Transposition of the subclavian artery to the common carotid artery
Prerequisite and indication
The subclavian artery is accessible via a supraclavicular approach, and
The distance between the subclavian and common carotid arteries is not too long for the transposition.
Carotidsubclavian Bypass (Fig. 12.4)
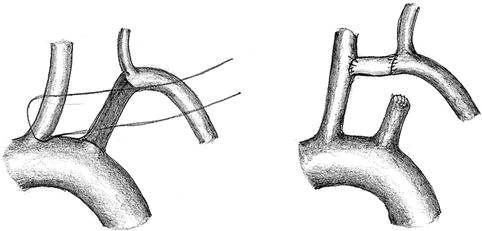
Fig. 12.4
Carotidsubclavian bypass
Prerequisite and indication
The subclavian artery is accessible via a supraclavicular approach.
Due to the long distance between the vessels a bypass graft is needed.
Carotidvertebral Bypass (Fig. 12.5)