Approach to Interpreting Abdominal and Pelvic Magnetic Resonance Imaging Examinations
Many radiologists and radiology trainees are intimidated by the prospect of interpreting abdominal and pelvic magnetic resonance imaging (MRI) studies, but such fear is unfounded. We remind our residents and fellows of two reassuring facts. First, the anatomy of the human body does not change with changes in imaging modality or scan plane. Second, the diseases of the human body remain the same, no matter how they are imaged. The pancreas is in the same location on a coronal MRI scan as it is on an axial computed tomography (CT) scan, although it is displayed differently. Likewise, there is a limited differential diagnosis for a cystic pancreatic mass, regardless of the modality used to image it.
Individuals new to abdominal and pelvic MRI should adopt a systematic approach. When faced with an abdominal or pelvic MR image, we recommend going through the following checklist:
Is the image T1- or T2-weighted? A T2-weighted image is easily identified by the presence of high signal intensity fluid within the spinal canal, bile ducts, or urinary tract. Using the signal intensity of fat to distinguish a T1- from a T2-weighted image is not recommended.
If the image is T1-weighted, is it in-phase or out-of-phase? This applies to gradient echo images. An out-of-phase image demonstrates phase cancellation at fat-water interfaces, resulting in a characteristic dark rim around the solid organs.
Is the image fat-suppressed or non-fat-suppressed?
Which direction is phase-encoded and which is frequency-encoded? This is important because one needs to be able to distinguish phase ghosts and other artifacts from actual lesions within the abdomen.
Are any artifacts present? Initially looking for artifacts such as phase ghosting, wraparound, and susceptibility artifact may prevent misinterpreting such artifacts later in the interpretive process.
Has intravenous contrast been administered? A fat-suppressed, T1-weighted, contrast-enhanced image may look similar to a fat-suppressed T2-weighted image (Fig. 3.1).
For contrast-enhanced images, what is the phase of enhancement (e.g., arterial, venous, equilibrium, delayed)?
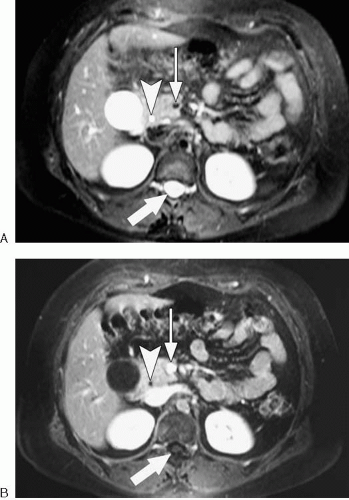 FIG. 3.1. Fat-suppressed T2-weighted images (A) may look similar to fat-suppressed, gadolinium-enhanced T1-weighted images (B). The bright cerebrospinal fluid (arrow) in (A) is clue that the image is T2-weighted. Note that common bile duct (arrowhead) is bright and superior mesenteric vein (thin arrow) is dark on T2-weighted image (A). Note that common bile duct (arrowhead) is dark and superior mesenteric vein (thin arrow) is bright on fat-suppressed, gadolinium-enhanced T1-weighted image (B). |
When an abnormality is seen, we recommend the following considerations:
In what organ or anatomic compartment is the abnormality located?
In which direction are adjacent organs or structures displaced?
Between what structures does the abnormality occur?Related posts:
 Basic Magnetic Resonance Imaging Principles for the Abdomen and Pelvis
Basic Magnetic Resonance Imaging Principles for the Abdomen and Pelvis
 Magnetic Resonance Cholangiopancreatography
Magnetic Resonance Cholangiopancreatography
 Magnetic Resonance Urography
Magnetic Resonance Urography
 Modifying Sequence Parameters
Modifying Sequence Parameters
 Glossary of Magnetic Resonance Imaging Terms
Glossary of Magnetic Resonance Imaging Terms
 What the Surgeon Needs to Know: Preoperative Assessment of Patients with Selected Tumors and Organ Transplant Candidates
What the Surgeon Needs to Know: Preoperative Assessment of Patients with Selected Tumors and Organ Transplant Candidates

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


