CHAPTER 6
Anorectum
INTRODUCTION
Management of diseases of the anorectum has traditionally been relegated to the proctologist, often a surgeon. The ease of sigmoidoscopy and the advent of video technology have provided the tools for endoscopists to assume a more active role in the evaluation and treatment of these disorders. Visual inspection of the perianal area coupled with digital examination should always precede endoscopic examination because subtle clues to underlying pathology may be identified. Retroflexion best permits evaluation of distal lesions, particularly those at or above the dentate line. A careful inspection of the anal canal should also be performed, especially for patients reporting anorectal pain and for patients with pain elicited on digital examination. Evaluation of the anal canal can also be performed with a disposable plastic anoscope.
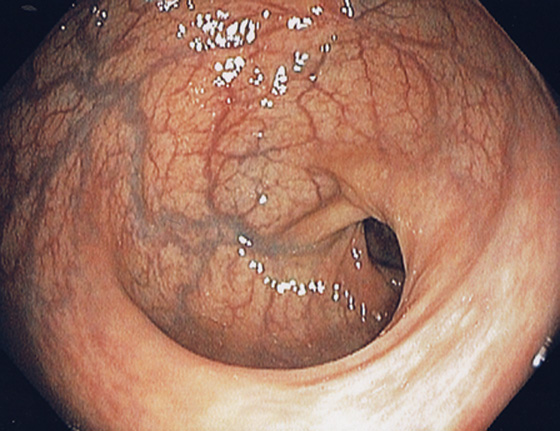
Figure 6.1 RECTUM
The rectum is characterized by prominent vascularity, in contrast with the sigmoid and proximal colon.
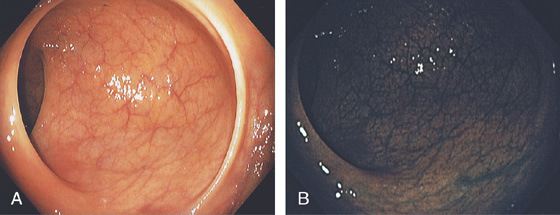
Figure 6.2 VALVES OF HOUSTON
A, The three valves of Houston are semilunar structures, two on the right and one on the left. In this patient in the left lateral decubitus position, the two valves on the right are anterior. B, Narrow band imaging demonstrates the subtle vascular pattern of the rectum.
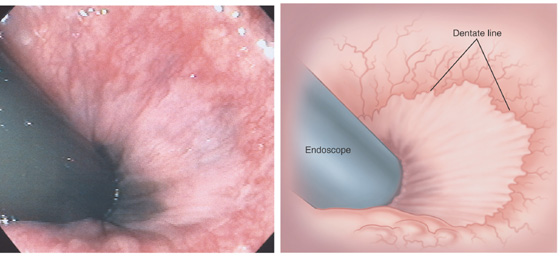
Figure 6.3 ANORECTAL JUNCTION ON RETROFLEXION
Retroflexion at the anorectal junction shows the dentate line demarcating the squamous mucosa from the colonic mucosa. In this case, black pigment of the squamous mucosa is near the endoscope.
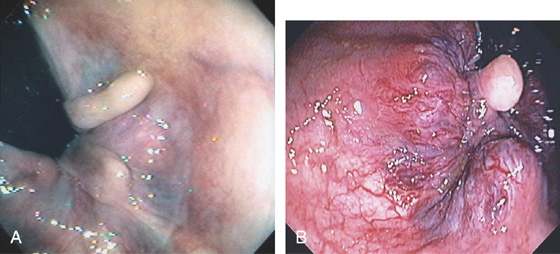
Figure 6.4 HYPERTROPHIED ANAL PAPILLAE
A, Three white polypoid structures are distal to the dentate line. These normal structures are hypertrophied, simulating a polyp on digital rectal examination. B, Solitary skin tag associated with enlarged hemorrhoidal tissue.
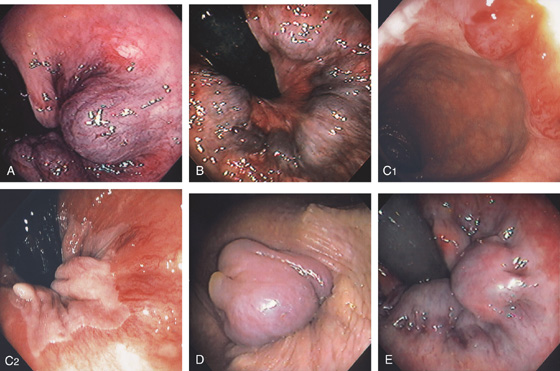
Figure 6.5 HEMORRHOIDAL DISEASE
INTERNAL HEMORRHOIDS
A, Although vascular cushions at the anorectum (hemorrhoids) are normal, this structure is markedly enlarged in this particular patient. The venous enlargement is proximal to the dentate line. B, Multiple internal hemorrhoids are at the dentate line. C1, Two reddish vascular tufts with overlying vasculature at the dentate line as seen on antegrade withdrawal of the colonoscope. C2, Retroflexed view confirms the location of the hemorrhoidal tissue proximal to the dentate line.
EXTERNAL HEMORRHOIDS
D, Thrombosed external hemorrhoid is shown. E, The enlarged vascular cushion is distal to the dentate line, thus representing an external hemorrhoid. The dentate line is well visualized.
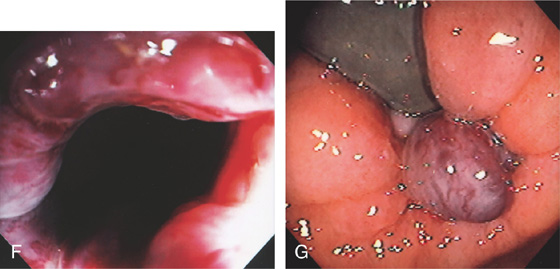
F, Multiple dilated veins on hemorrhoidal tissue are similar to the red signs on esophageal varices. G, External hemorrhoid prolapsed back in the rectum as shown on retroflexion.
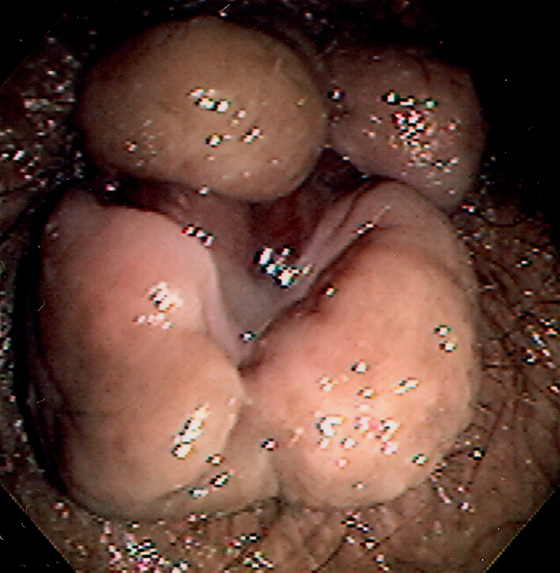
Figure 6.6 EXTERNAL HEMORRHOIDS IN PORTAL HYPERTENSION
Prominent external hemorrhoids in a patient with cirrhosis, portal hypertension, and esophageal varices.
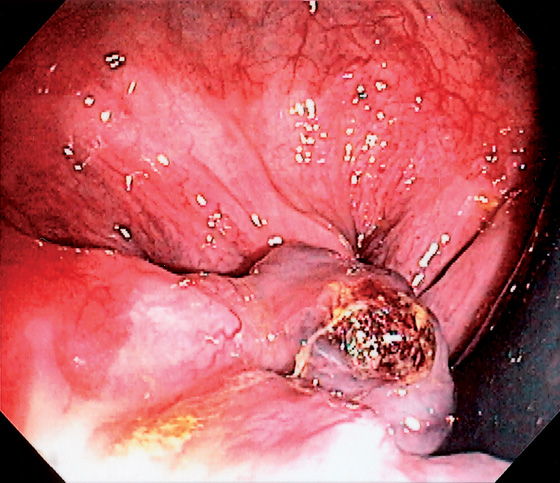
Figure 6.7 EXTERNAL HEMORRHOID WITH BLEEDING STIGMATA
Note the adherent blood clot on the external hemorrhoid as shown on retroflexion.
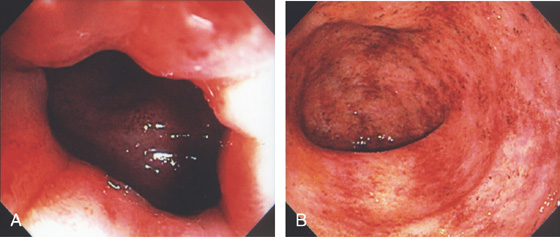
Figure 6.8 ULCERATIVE PROCTITIS
A, The colitis can be seen to begin just inside the anal verge. B, Marked proctitis with all the features of colitis including loss of the mucosal vascular pattern, edema, subepithelial hemorrhage, friability, and mucopus.
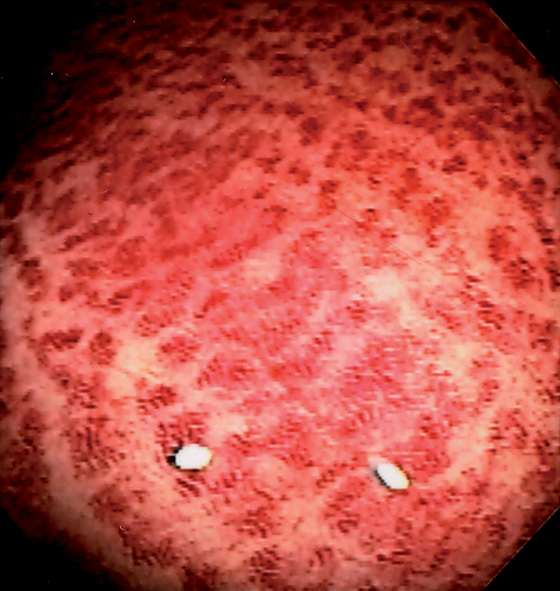
Figure 6.9 NONSPECIFIC HEMORRHAGE
Striking subepithelial hemorrhage in the rectum. Biopsies disclosed no specific cause. Such nonspecific changes can be seen in patients on anticoagulation, or who have thrombocytopenia, or the changes lack specific explanation.
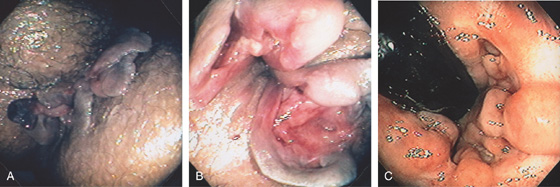
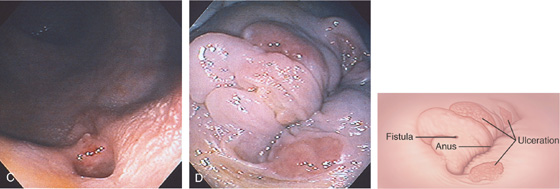
Figure 6.10 PERIANAL CROHN’S DISEASE
A, Multiple large skin tags at the anus simulate thrombosed external hemorrhoids. B, Further inspection reveals fistulae at the base of the tags. Fistulae are also seen in areas of ulcerated mucosae. C, Retroflexion at the anorectal junction demonstrates multiple serpiginous ulcerations, typical of Crohn’s disease.

Figure 6.11 MULTIPLE SKIN TAGS IN CROHN’S DISEASE
Multiple skin tags at the anal verge in a patient with long-standing Crohn’s disease.
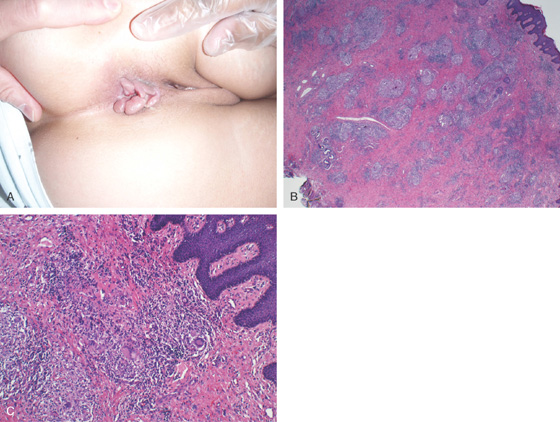
Figure 6.12 MULTIPLE SKIN TAGS IN CROHN’S DISEASE
A, Multiple ulcerated skin tags. B, After surgical resection, granulomas can be seen, as well as multinucleated giant cells (C).
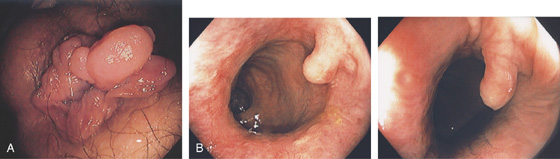
Figure 6.13 SKIN TAGS FROM PRIOR HEMORRHOIDAL DISEASE
A, Multiple skin tags and redundant tissue at the anal verge caused by prior hemorrhoidal disease. B, Solitary large skin tag at the dentate line as shown on antegrade view.
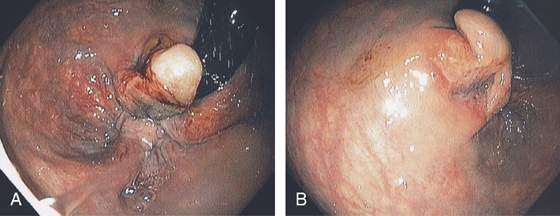
Figure 6.14 BLEEDING SKIN TAG
A, Retroflexed view shows a large skin tag with fresh bleeding. B, After washing, ulceration can be seen at the base of the large skin tag.
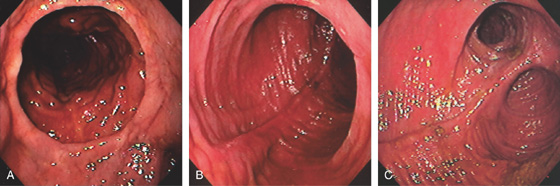
Figure 6.15 J POUCH
A, Distal anastomosis in the foreground. B, Characteristic appearance of the pouch. C, Both limbs are now shown.
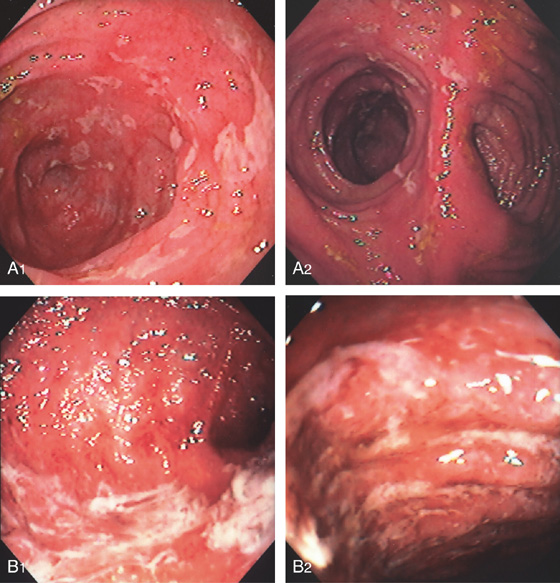
Figure 6.16 POUCHITIS
Patchy ulceration and edema in the pouch extending to the limbs (A1, A2). B1, B2, More diffuse disease with edema, ulcerations, and mucopus.
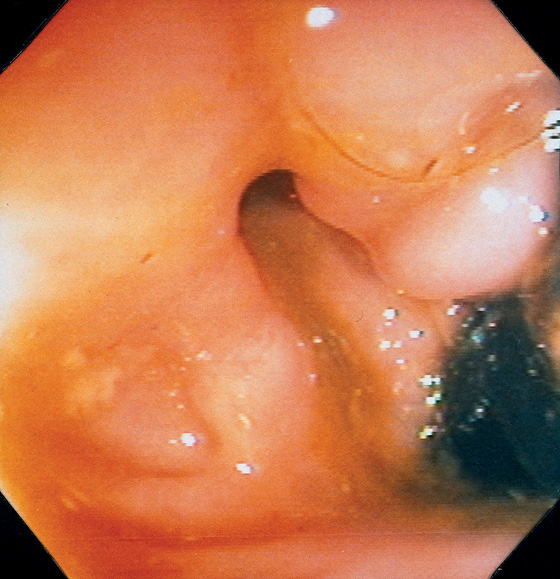
Figure 6.17 RECTAL FISTULA
Retroflexion in the rectum demonstrates an opening near the anorectal junction. This patient had a history of Crohn’s disease. Note the absence of rectal inflammation. The fistula could also be identified in the antegrade view of the anorectum.
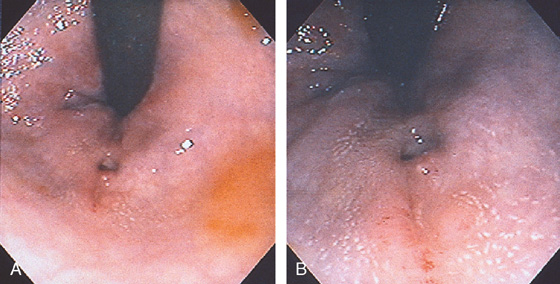
Figure 6.18 RECTAL AND PERIANAL FISTULAE
Fistulous opening proximal to the dentate line on retroflexion view (A, B).
Opening is shown antegrade on withdrawal (C). Perianal skin tags with erosions and a fistulous opening are also noted (D).
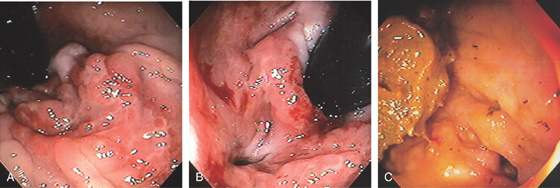
Figure 6.19 RECTAL FISTULA IN CROHN’S DISEASE
A, Ulceration at the anal verge in a patient with Crohn’s disease. B, Fistula site identified. C, After medical therapy, the rectal mucosa is now normal, although the fistula is still widely patent. This patient now reported passage of stool through the vagina.
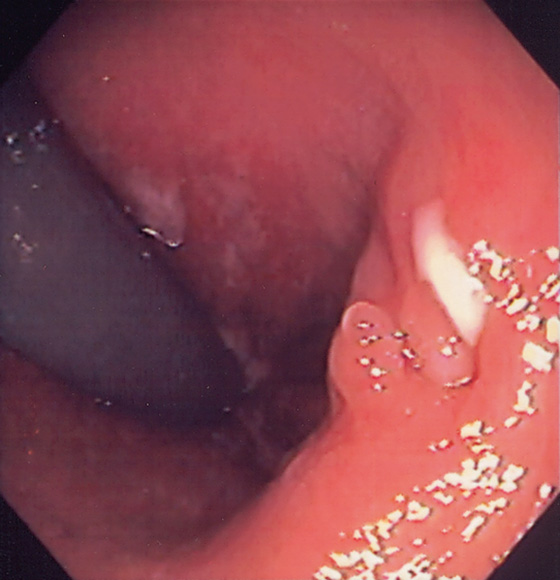
Figure 6.20 RECTAL FISTULA
Area in the distal rectum as shown on retroflexion with nodularity and where pus was seen to pass spontaneously.
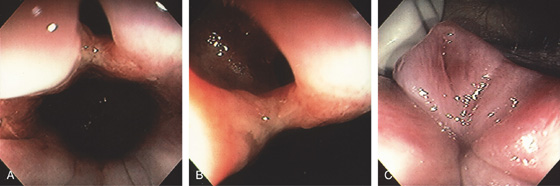
Figure 6.21 FISTULA IN ANO
A, Opening in the anal canal. B, Close-up shows the fistula. C, Redundant tissue at the anal verge with an opening representing the fistulous tract.
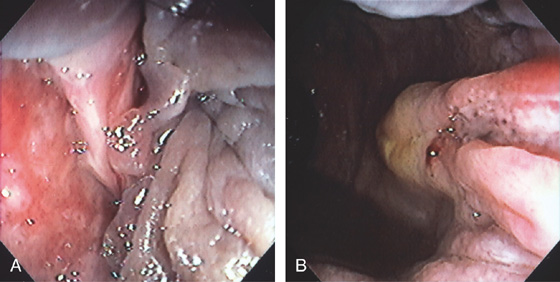
Figure 6.22 FISSURE
Linear tear in the anal canal with associated sentinel pile (A, B).
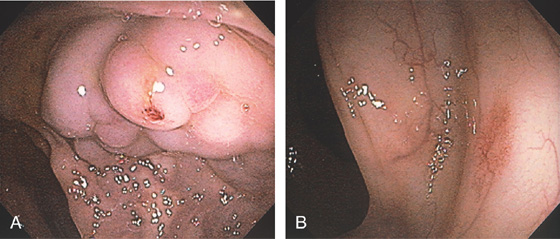
Figure 6.23 RECTAL VARICES
A, Cluster of varices in the distal rectum. There is bleeding stigmata on one of the variceal trunks. B, A vascular ectasia was identified just proximal to the varices. These can be seen in colonic disease related to portal hypertension.
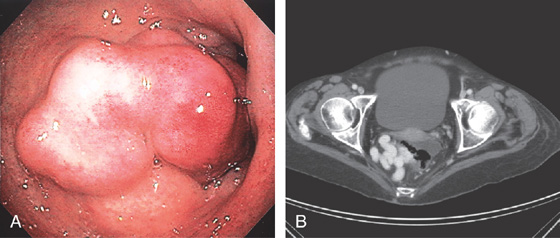
Figure 6.24 RECTAL VARICES
A, Large cluster of veins in the midrectum resembling a mass lesion. B, Contrast examination shows a large variceal trunk in the rectum.
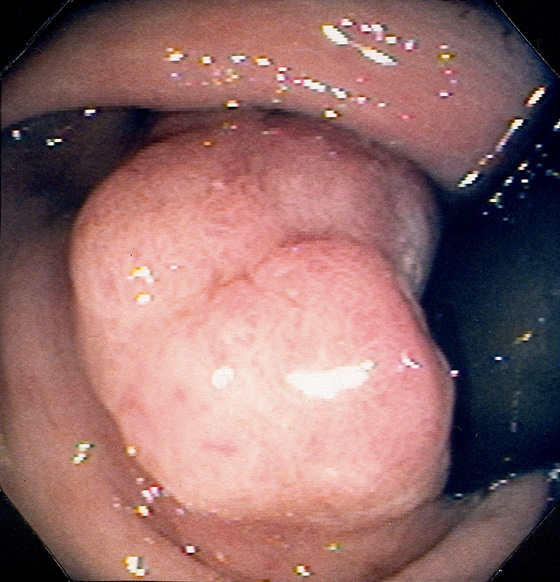
Figure 6.25 ADENOMATOUS POLYP
Large, adenomatous-appearing polyp at the anorectal junction shown on retroflexion. A soft mass lesion was palpated on digital rectal examination. The lesion could not be observed as the endoscope was advanced into the rectum.
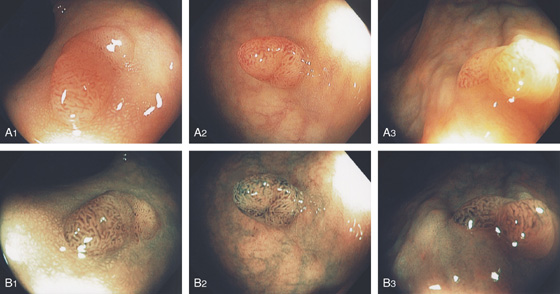
Figure 6.26 ADENOMATOUS POLYP
A1-A3, Typical-appearing small sessile polyp in the distal rectum on standard and narrow band imaging (B1-B3).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


