, Ivan Damjanov1 and Ryan M. Taylor2
(1)
University of Kansas School of Medicine, University of Kansas, Kansas City, KS, USA
(2)
Division of Gastroenterology and Hepatology, University of Kansas School of Medicine, Kansas City, KS, USA
Handling and processing of the liver biopsy includes the following steps:
Gross examination and identification
Fixation
Embedding in paraffin and sectioning
Staining of the sections
Special stains
Additional studies, as indicated
Histologic Processing
Gross examination of the biopsy specimen removed from the biopsy needle is usually of limited value diagnostically. Nevertheless it should be part of the entire procedure and to assure proper identification of the specimen. Statistics show that a small number of specimens labeled as liver biopsies are actually not composed of liver tissue and contain only skeletal muscle, lungs, kidney, fat and connective tissue or just clotted blood. Such biopsies containing non-hepatic tissue could be immediately repeated to obtain adequate amounts of liver tissue.
The liver tissue is normally brown, but if congested it may be red. Green color is usually a sign of cholestasis, and yellow color is typical of fatty change. Dark brown tissue is seen in hemochromatosis. In Dubin-Johnson syndrome the liver tissue is also dark brown or even black. Biopsies composed of fibrous tissue and stroma rich tumors or squamous cell carcinomas are usually white.
Fixation includes immersion of liver biopsy tissue in 10 % formalin for a minimum of 2–4 h. The specimen should be handled gently to avoid compression artefacts and immersed in fixative as soon as possible. Samples submitted in saline or wet gauze will show substantial artefactual changes and are considered to be suboptimal for proper diagnosis if not outright unacceptable by most pathologists.
Routine and Special Stains
The specimen is embedded into paraffin and sectioned at a thickness of 3–6 μm. The sections are deparaffinized and routinely stained with hematoxylin and eosin. In addition most laboratories stain parallel sections with a trichrome stain (usually according to Masson), Perl’s iron stain, periodic acid Schiff (PAS) reaction, with and without predigestion with diastase (Figs. 1, 2, 3, and 4). Many laboratories include also reticulin stain (Fig. 5). Congo red stain is used if amyloidosis is suspected, and rhodanine for identification of copper in Wilson disease. Commonly used special stains are listed in Table 1.
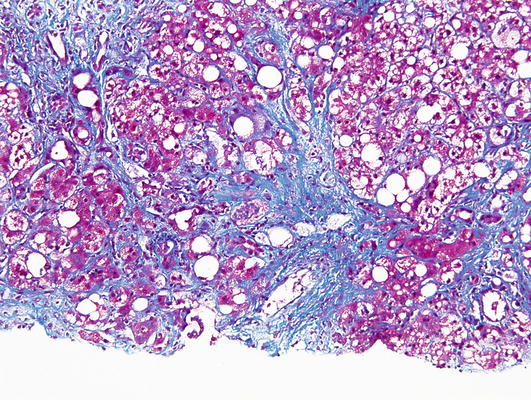
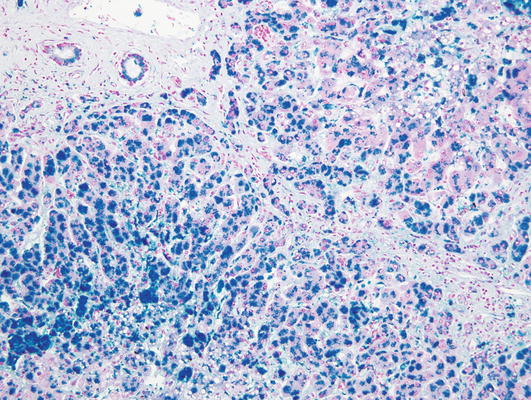
Fig. 1.
Trichrome stain. Masson’s trichrome stains the connective tissue blue in this biopsy of a liver affected by advanced steatohepatitis
Fig. 2.




Perl’s iron stain. Hemosiderin appears blue
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
