Adrenals
ANATOMY
The adrenal glands are two small, triangular, retroperitoneal structures, weighing 3 to 5 g, with a fascial covering provided by a superior extension of Gerota’s fascia. The right adrenal blood supply comes mainly from the inferior adrenal artery off the right renal artery, the middle adrenal artery off the aorta, and the superior adrenal artery off the inferior phrenic. The left adrenal blood supply comes mainly from the middle adrenal artery arising from the aorta and smaller superior and inferior adrenal arteries. The very short right adrenal vein empties directly into the vena cava, whereas the left adrenal vein empties into the left renal vein, lateral to the aorta and medial to the gonadal. Lymphatic drainage of both glands is primarily to the lateral aortic lymph nodes just above the level of the renal arteries and anterior to the crura of the diaphragm.
PHYSIOLOGY
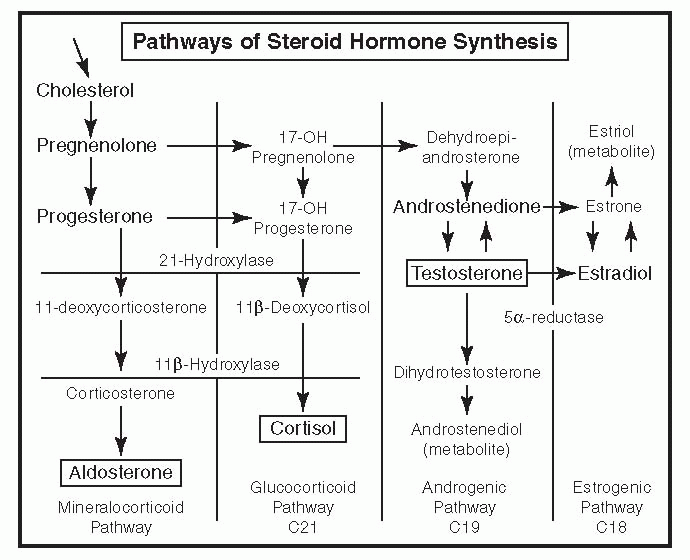
The outer cortical zona glomerulosa produces aldosterone under the influence of angiotensin II and the renin-angiotensin system (see “Renin-Angiotensin-Aldosterone system” in Chapter 31) and directly by serum potassium. Aldosterone acts at the distal tubule to cause sodium retention and potassium secretion. Hyperkalemia is an important independent stimulus to aldosterone secretion.
The middle zona fasciculata and inner zona reticularis secrete primarily cortisol and dehydroepiandrosterone (DHEA) under the influence of pituitary adrenocorticotropic hormone (ACTH). Pituitary ACTH is under continuous feedback inhibition by cortisol. 17-Ketogenic steroids (17-KGS) are metabolites of cortisol, whereas 17-ketosteroids (17-KS) are metabolites of adrenal androgens (DHEA).
The adrenal medulla chromaffin cells function as a giant presynaptic sympathetic nerve ending secreting catecholamines,
norepinephrine (20%), and epinephrine (80%). Vanillylmandelic acid (VMA) is a major catecholamine degradation product formed by the combined action of catechol-O-methyl transferase and monoamine oxidase.
norepinephrine (20%), and epinephrine (80%). Vanillylmandelic acid (VMA) is a major catecholamine degradation product formed by the combined action of catechol-O-methyl transferase and monoamine oxidase.
|
PATHOLOGY
Cushing’s Syndrome
Cushing’s syndrome is a clinical entity characterized by plethoric facies, bruising, truncal obesity, change in appearance, purplish cutaneous striae, hypertension, osteoporosis, hypokalemia, and poor wound healing as a result of hypersecretion of cortisol. A 24-hour urine demonstrating hyperexcretion of cortisol is the most reliable test. Exogenous steroid administration is the most common cause of hypercortisolism and should be ruled out first.
▪ Etiology
Cushing’s Disease (75%)
Ectopic Adrenocorticotropic Hormone (<5%)
Extra-adrenal ACTH-producing tumors are unresponsive to cortisol negative feedback and arise from malignant carcinomas in the lung, breast, ovary, gastrointestinal tract, and kidney. Most common are oat cell bronchogenic carcinomas, thymic tumors, or islet cell tumors of the pancreas. Treatment is surgical excision of the tumor.
Adrenal Adenoma (10%)
This condition presents with autonomous hypersecretion of cortisol and low serum ACTH levels. These are occasionally adenocarcinomas that are radioresistant and unresponsive to chemotherapy. Adrenal adenomas are generally 2 to 5 cm, whereas adrenal carcinomas are usually >6 cm. Treatment is radical adrenalectomy and lymphadenectomy.
Aldosteronoma (Conn’s Syndrome)
Aldosterone hypersecretion owing to an adrenal adenoma or hyperplasia is characterized by hypertension, hypokalemic alkalosis, and low plasma renin activity (PRA). Aldosteronomas are small tumors, usually <3 cm, occurring between age 30 and 60 years and are more common in females than males (2:1). Primary hyperaldosteronism accounts for <1% of all cases of hypertension.
▪ Major Criteria for Diagnosis
Hypertension
Hypokalemia in the absence of diuretics
High aldosterone output in the setting of high sodium intake
Suppressed plasma renin levels that fail to rise under conditions of upright position and restricted sodium intake
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


