Upon entry into the left hemithorax, the six key goals of resuscitative thoracotomy include:
1. Confirmation of ETT placement
2. Direct control of intrathoracic hemorrhage
3. Pericardiotomy and release of tamponade
4. Cross clamping of the thoracic aorta
5. Open cardiac massage
6. Evacuation of air embolism
3.4 Management of Specific Injuries
3.4.1 Cardiac
The primary goals in the management of cardiac injuries identified at resuscitative thoracotomy are to relieve pericardial tamponade and control hemorrhage. To this end, digital occlusion of the injury followed by cardiorrhaphy using a running continuous suture of 2-0 to 4-0 polypropylene is a rapid means of obtaining immediate hemostasis. There should be a low threshold for extending the incision to the contralateral hemithorax and performing a clamshell thoracotomy, particularly if lack of accessibility or visualization of injuries impedes surgical hemostatic efforts (Fig. 3.1). It is imperative to ligate the internal mammary arteries following a clamshell thoracotomy.

Fig. 3.1
Clamshell thoracotomy in a patient with multiple bilateral stab wounds
Balloon catheter tamponade using a Foley catheter (18 Fr) that is placed in the wound, inflated, and put on traction to fill the defect is an alternative method of obtaining rapid hemostasis (Fig. 3.2) [5]. Following placement of sutures, the Foley catheter is deflated and removed prior to securing the repair. Temporary release of traction on the Foley catheter during suture placement may help avoid the inadvertent error of placing a suture through the Foley catheter.
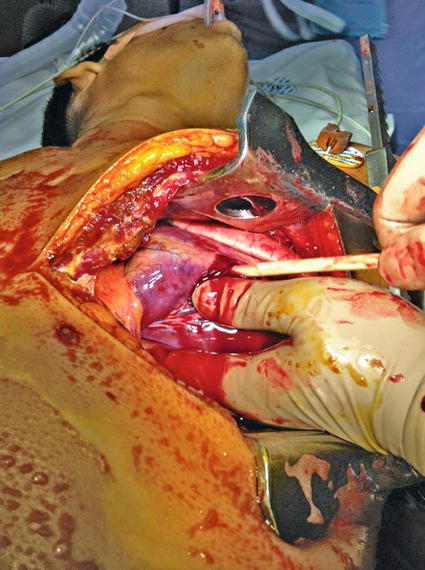
Fig. 3.2
Foley catheter tamponade of a gunshot wound to the right ventricle
The use of standard skin staplers has been advocated for the temporary closure of penetrating cardiac wounds, particularly in patients with large wounds or multiple injuries that would be otherwise difficult to control using standard suture closure techniques [6]. In addition to being rapid and effective, skin staplers may also reduce the risk of contamination associated with attempted suture hemostasis during resuscitative thoracotomy.
3.4.2 Vascular
Thoracic vascular injuries are uncommonly encountered injuries and may thus present a formidable challenge to even the most experienced of trauma surgeons. For patients sustaining a penetrating injury to the thoracic outlet, a high index of suspicion must be maintained for the presence of major vascular injury. In patients with supraclavicular wounds accompanied by intra- or extrathoracic hemorrhage, balloon catheter tamponade has been demonstrated to be an effective and rapid means of obtaining temporary hemorrhage control [7]. Patients with a suspected venous injury should be placed in the Trendelenburg position to decrease the risk of air embolism.
As most patients will have undergone a resuscitative thoracotomy, direct pressure using lap pads in conjunction with efforts to obtain proximal and distal control remains the mainstays of early operative management, with or without direct repair, if possible. For patients with subclavian or axillary vessel injuries, distal control via a separate curvilinear clavicular incision including disarticulation or resection of the clavicle may be required. Distant intraluminal vascular control with the use of Fogarty catheters, the use of temporary intravascular shunts, and ligation are other damage control options that have been successfully used [8]. Injury to the thoracic aorta should be managed with a combination of partial clamping and lateral arteriorrhaphy with consideration given to extracorporeal life support in injuries not amenable to direct repair. Other options include intravascular shunt placement using a chest tube. Injuries to the vena cava and azygous vein can be managed via venorrhaphy or ligation, when necessary. Intercostal vessel bleeding may be a frustrating source of bleeding particularly if located posteriorly or inferiorly. Judicious use of counter incisions overlying the affected rib space may facilitate efforts to obtain proximal and distal suture ligature control.
3.4.3 Pulmonary
Lung-sparing techniques have become the standard approach to the management of pulmonary parenchymal injuries. Suture pneumonorrhaphy may be a useful technique for obtaining hemostasis in superficial lacerations of the lung parenchyma. Nonanatomic resection in the form of stapled wedge resection, particularly for peripherally located injuries, may be rapidly performed [9]. For through-and-through injuries to the lung, stapled pulmonary tractotomy (using a standard linear GIA stapler) with selective vascular ligation is associated with improved outcomes including decreased operative time and blood loss, as well as parenchymal salvage when compared to anatomic resections such as lobectomy [10]. Recently, argon beam coagulation (ABC) has been demonstrated to be a useful adjunct for hemorrhage control in pulmonary tractotomy [11].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


