Fig. 2.1
Seat belt injury to the left flank
As the next step in the work-up after the clinical examination, two imaging studies should be ordered: Ultrasound and computed tomography (CT) can both be performed quickly and efficiently, but once again, it must be borne in mind that only a stable trauma patient can undergo CT.
Ultrasound can readily be performed in the emergency room. Rozycki’s Focused Assessment for the Sonographic Examination of the Trauma Patient (FAST) protocol was designed to determine the presence of free fluid in the abdominal cavity and assess its quantity and location [1]. With handheld portable equipment, FAST is noninvasive and non-stressful. It can be repeated as necessary and can be performed simultaneously without sedation with ongoing resuscitation, and even at bedside. Rozycki et al. reported a sensitivity of 83.3 % and specificity of 99.7 % in 1,540 patients with blunt and penetrating injuries [10].
CT can provide valuable supplemental information on morphologic changes in solid organs, with 97 % sensitivity, 98 % specificity, and 98 % accuracy for peritoneal violation [11]. In detecting bowel injury, CT has an overall sensitivity of 94 %, and 96 % in detecting mesenteric injury [7].
Unlike CT, ultrasound requires an experienced sonographer. Both ultrasound and CT are of limited value in diagnosing injuries to the diaphragm: Mihos et al. [9] achieved a correct preoperative diagnosis in only 26 % of 65 patients with a diaphragmatic injury; in 74 % the diagnosis was only made during the operation.
2.3 Why Do We Need Laparoscopy in Trauma?
Even with the high-quality information that these two noninvasive methods provide, it can be difficult to diagnose blunt abdominal trauma. Misleading negative results can have serious consequences, especially when the gastrointestinal tract and pancreas are involved, but if exploratory laparotomies are performed routinely when there is the least suspicion of visceral trauma, morbidity rates and costs will increase unnecessarily.
Fortunately, there are well-delineated scenarios that define the place of laparoscopy in the diagnosis and treatment of visceral trauma, blunt, or penetrating.
Villavicencio and Ancar reported that screening by laparoscopy for blunt trauma was associated with a sensitivity of 90–100 %, a specificity of 86–100 %, and accuracy of 88–100 % [14]. In nine prospective series, screening laparoscopy for penetrating trauma showed sensitivity of 85–100 %, specificity of 73–100 %, and accuracy of 80–100 % with two procedure-related complications among 543 patients [11]. Diagnostic laparoscopy for blunt trauma had a sensitivity of 100 %, specificity of 91 %, and accuracy of 96 %; for penetrating trauma sensitivity was 80–100 %, specificity 38–86 %, and accuracy of 54–89 % [15]. The rate of missed injuries upon laparoscopy was 0.4 % (6 of 1,708 patients). The rate of laparoscopy-related complications was 1.3 % (22 of 1,672 patients) [15]. Laparoscopy may allow laparotomy to be avoided in up to 63 % of patients presenting with a variety of injuries [15]: A negative laparotomy will be circumvented in 23–54 % of patients with stab wounds and blunt abdominal trauma [3]. In any case, laparoscopy is more cost-effective than negative laparotomy [12].
2.4 Selection of Patients
Patients should only undergo laparoscopy when, in spite of prior imaging studies, there is no obvious indication for laparotomy but an unclear diagnosis requires further investigation. Once again, all patients with blunt or penetrating trauma considered for laparoscopy must be hemodynamically stable, or become so rapidly after resuscitation.
2.5 Indications for Laparoscopy
Diagnostic and/or therapeutic laparoscopy can be indicated in the following settings:
Get Clinical Tree app for offline access

1.
Blunt Trauma
(a)
Unclear abdomen after blunt trauma. “Unclear abdomen” means that there is a discrepancy between the clinical findings and imaging studies. If, in spite of conservative measures, symptoms are diffuse and do not improve, laparoscopy has the potential to clarify the situation quickly and may also allow therapeutic measures to be implemented.
(b)
Free fluid from an unclear source. Stable patients with free fluid in the peritoneal cavity following blunt abdominal trauma can be treated conservatively unless the situation escalates with more free fluid and abdominal symptoms. These cases are usually due to a mesenteric laceration that CT scan has missed (Fig. 2.2).

Fig. 2.2
Mesenteric injury not diagnosed by CT but detected during laparoscopic exploration
(c)
Suspected intestinal injury. When the extent of injury/perforation (overt or covert), ischemia, necrosis, and/or ongoing bleeding cannot be determined with certainty from ultrasound and/or CT scan, laparoscopy is the best option to obtain a positive or negative diagnosis. A further advantage is that therapeutic measures such as oversewing a laceration or performing a resection can be undertaken during the procedure.
(d)
Injury to the mesentery with or without associated vascular damage to the intestine. Even when CT suggests one or more mesenteric lacerations, it is often difficult to determine whether the involved segment of the intestine is adequately perfused or is ischemic or necrotic. Here, laparoscopic exploration can locate and visualize the injury and assess intestinal vitality, so that suitable measures can be taken (Fig. 2.3).
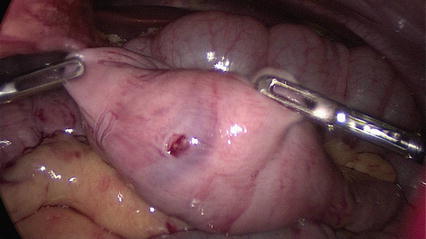
Fig. 2.3
Stab injury to the bowel undetectable by CT scan
(e)
Blunt Trauma – solid organ injury. Lesions to the pancreas tend to be surreptitious and escape detection with ultrasound and CT studies. When revealed by laparoscopy, they can be debrided and drained.
2.
Penetrating Trauma
In the stable patient, laparoscopy allows determination of peritoneal penetration and subsequent exploration of the abdomen for other organ injuries (Fig. 2.4). In the same session it may be possible to treat penetrating injuries to hollow organs such as the stomach or intestines. An additional advantage of laparoscopic exploration in the patient with a thoracoabdominal stab or gunshot wound in the flank is the detection of diaphragmatic lesions that often go unseen on CT. In these patients, laparoscopic or thoracoscopic exploration is ideal to determine whether repair should be undertaken immediately or another approach (laparotomy or thoracotomy) would be more suitable.