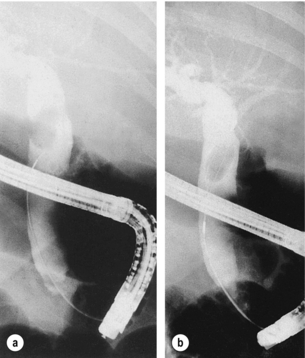
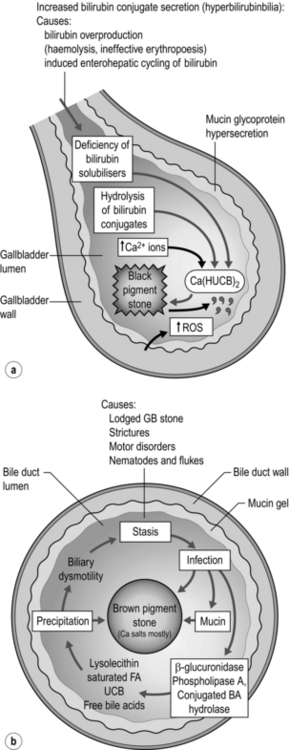
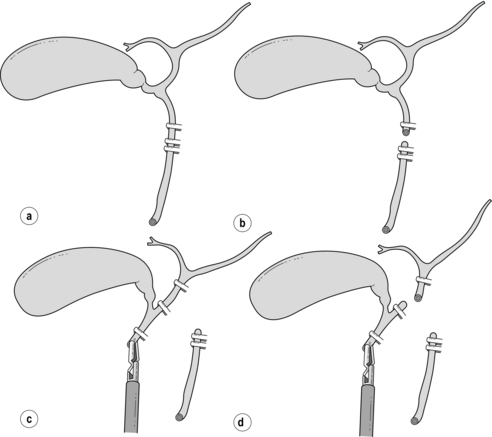
10 In the UK it has been estimated from autopsy studies that approximately 12% of men and 24% of women of all ages have gallstones present.1 The prevalence in North America is comparable to that in the UK, and it is believed that 10–30% of gallstones become symptomatic. There is a high prevalence in native Americans, who have an incidence of 50% in men and 75% in women in the age group 25–44 years, and this points to the importance of genetic factors in the aetiology of gallstones. In the UK more than 40 000 cholecystectomies are performed each year,2 whereas in the USA approximately 500 000 operations are performed annually.3 The incidence of common bile duct stones found before or during cholecystectomy is approximately 12%,4 indicating that in the UK alone more than 4000 common bile ducts require stone clearance annually. Gallstones are usually designated as cholesterol stones, mixed stones or pigment stones.5 Pure cholesterol and pure pigment stones account for only 20% of gallstones, and mixed stones are considered as variants of cholesterol stones as they usually contain over 50% cholesterol and account for about 80% of gallstones in Western countries. Chemical analysis shows a continuous spectrum of stone composition rather than three mutually exclusive stone types, and 10–20% contain enough calcium to be rendered radio-opaque. The two most important determinants of gallstone frequency in any population are age and gender; gallstones become more common with increasing age and are at least twice as common in women.6 The increased frequency in women becomes manifest at puberty, and an increased risk of gallstones is conferred by parity and by the ingestion of oral contraceptives.7 Other factors related to the development of cholesterol gallstones include obesity, ileal disease or resection, cirrhosis, cystic fibrosis, diabetes mellitus, long-term parenteral nutrition, impaired gallbladder emptying, ingestion of clofibrate,8 heart transplant,9 and periods of dieting on a very low fat diet.10 A positive family history of previous cholecystectomy also increases the risk of developing symptomatic gallstone disease.11 Increasing evidence is emerging that impaired colonic motility contributes to stone formation, and speculation arises for this as a means of prevention.12 Pigmented gallstones are composed mainly of calcium hydrogen bilirubinate, in a polymerised and oxidised form in ‘black’ stones and in unpolymerised form in ‘brown’ stones. Black stones form in sterile gallbladder bile, but brown stones form secondary to stasis and anaerobic infection in any part of the biliary tree (Fig. 10.1). Figure 10.1 Schematic outline of the pathogenesis of ‘black’ pigmented stones in sterile gallbladder bile (a) and ‘brown’ pigmented stones in an obstructed biliary tree (gallbladder infrequently) infected with a mixed anaerobic microflora derived from the colon (b). Adapted from Vitek L, Carey MC. New pathophysiologic concepts underlying pathogenesis of pigment gallstones. Clin Res Hepatol Gastroenterol 2012; 36(2):122–9. Brown stones form in any part of the biliary tree from any cause of chronic stasis and anaerobic infection. Anaerobes secrete enzymes that hydrolyse ester and amide linkages in biliary lipids into calcium-sensitive anions that phase separately as insoluble anions or calcium salts. These precipitates deposit on obstructing elements such as small cholesterol crystals, black stones from the gallbladder, parasite eggs and dead worms or flukes. Oriental hepatolithiasis syndrome is the most serious manifestation of brown pigment stone disease.13 It is uncertain whether all common bile duct (CBD) stones produce symptoms. It is traditionally held that the CBD cannot produce colicky pain as it does not contain smooth muscle, but pain in the right upper quadrant following cholecystectomy may be a sign of retained bile duct stones. A stone impacted in the lower end of the CBD may also be associated with nausea and vomiting, and undoubtedly the muscular spasms of the sphincter of Oddi or duodenum could account for the pain that is often felt radiating through to the back. Obstructive jaundice results when a stone becomes impacted within the CBD, in the tapered portion within the pancreas or ampulla. A stone may pass spontaneously or fall back into the CBD (‘ball-valving’) with spontaneous regression of the jaundice, or it may remain impacted until it is removed. A stone at the lower end of the CBD may also cause pancreatitis by temporary obstruction of the pancreatic duct, and this may be associated with transient jaundice (see Chapter 13). Ascending cholangitis results from infection within an obstructed or poorly draining biliary system. In patients with CBD stones, coliforms are identified within the bile in around 80% of cases.14 The classic Charcot’s triad of symptoms produced by bile duct stones with cholangitis consists of pain, obstructive jaundice and fever (with or without rigors). Acute cholangitis may progress to acute obstructive suppurative cholangitis with pain, obstructive jaundice, fever, hypotension and mental obtundation (Reynolds’ pentad) requiring early recognition and prompt endoscopic retrograde cholangiopancreatography (ERCP) drainage to save life.15 Liver function tests (LFTs) should be performed routinely in patients with suspected gallstones. Although these may not be affected by the presence of cholecystolithiasis, they may be abnormal in the presence of choledocholithiasis. An isolated increase of unconjugated bilirubin is present in prehepatic jaundice such as is seen with excessive haemolysis. The biochemical picture of hepatic jaundice, as seen with hepatitis, is one of raised conjugated and unconjugated bilirubin, high aspartate (AST) and alanine (ALT) transaminase levels, but associated with a relatively normal or slightly raised alkaline phosphatase (ALP). Posthepatic (obstructive) jaundice is associated with a raised conjugated bilirubin only, high ALP, and normal AST and ALT. In late cases of obstructive jaundice or in acute cholangitis, the transaminase levels will rise as hepatocellular damage proceeds. Minor abnormalities in the LFTs occur with non-obstructing stones in the CBD. These minor abnormalities may prompt the undertaking of an operative cholangiogram at the time of surgery if a selective operative cholangiogram policy is being pursued.16,17 Approximately 60% of patients with CBD stones (including asymptomatic stones) will have one or more abnormal LFTs, although a substantial number of patients with an abnormal LFT will not have CBD stones. Bilirubin, ALP and γ-glutamyl transpeptidase (GGT) are the most sensitive tests routinely used.18 In the acute situation, a serum amylase or lipase level should also be ascertained to exclude a diagnosis of pancreatitis, and a raised white blood cell count may support a clinical diagnosis of acute cholecystitis. Ultrasound is the investigation used most widely to confirm the diagnosis of cholelithiasis. It is easy to perform, causes little discomfort to the patient, avoids irradiation and potentially toxic contrast media, and may be useful in demonstrating and assessing other structures in the upper abdomen. The gallbladder wall, as well as its contents, can be assessed and this may give additional information useful for planning management. CBD stones may be harder to identify, although the presence of a dilated CBD and small stones within the gallbladder give clues as to their presence. If the gallbladder cannot be identified, the presence of an echogenic focus in the gallbladder area is nearly as specific a finding as that of calculi in a distended gallbladder. With high-quality ultrasound scanning, gallstones should be detected in at least 95% of patients with stones. Its reliability in detecting CBD stones varies between 23% and 80% depending on body habitus and experience of the ultrasonographer.19 Prat et al. have reported EUS with a sensitivity of 93% and specificity of 97% in detecting CBD stones, showing some promise of approaching values achieved by ERCP (89% and 100%).20 EUS has also been reported as more sensitive than the transabdominal approach. Norton and Alderson reported confirmation of gallstone disease in 15 of 44 patients with ‘idiopathic’ pancreatitis who underwent EUS.21 CT may be more accurate than ultrasound in identifying CBD stones, with a sensitivity of 75% for CBD stones causing obstructive jaundice.22 However, the relatively low rate of gallbladder stone detection may be due, in part, to cholesterol stones being isodense with bile on CT. The newer generation spiral CT and magnetic resonance imaging (MRI) may be better but their potential advantage over abdominal ultrasound scanning is not readily apparent. Spiral CT following intravenous infusion cholangiography has been shown to allow accurate reconstruction of cystic duct/CBD anatomy and providing severe jaundice is not present rivals magnetic resonance cholangiopancreatography (MRCP) in its capacity to outline CBD stones.23 Fast image acquisition in a few seconds and improved software have allowed imaging of the biliary and pancreatic tree in enough detail to approach the resolution of ERCP.24 The technique relies on the principle of imaging fluid columns that are static and so give detail of bile and static fluid in the duodenum and stomach. Better images are obtained with dilated ducts, and bile flow can be a source of error in false-positive stone detection. The presence of CBD calculi can be detected with a sensitivity of 95%, specificity of 89% and accuracy of 92%. The ability to detect anatomical variation of the extrahepatic bile ducts is less established.25 Following standard non-invasive tests, Liu et al. stratified suspicion of CBD stones into four categories. Patients at extremely high risk of CBD stone underwent ERCP. Patients at high risk underwent MRCP followed by ERCP if stones were seen. With diagnostic accuracies greater than 90% many patients were spared unnecessary ERCP.26 ERCP is considered the gold standard in preoperative CBD imaging. With direct visualisation of the papilla using a side-viewing duodenoscope, the papilla can be cannulated selectively to provide images of both the pancreatic and common bile ducts. Water-soluble contrast medium is injected to outline the biliary tree, and offers the advantage over other biliary tree imaging techniques of therapeutic intervention with sphincterotomy and stone extraction at the time of examination (Fig. 10.2). The role of ERCP in the management of CBD stones is discussed later in this chapter. There has been much debate regarding the need for surgical intervention in patients with asymptomatic gallstones. In one American study, which assessed the natural history of subjects with asymptomatic stones, individuals with gallstones were diagnosed by ultrasound scan on entry to a large university healthcare plan.27 Only 2% of patients with incidentally diagnosed gallstones became symptomatic each year and presented with biliary colic or cholecystitis rather than the more serious complications of jaundice, empyema or cholangitis.27 Only 10% of the asymptomatic patients, followed for a mean of almost 5 years by McSherry and Glenn, developed symptoms, and only 7% required operation.28 Although stones are undoubtedly associated with an increased risk of gallbladder cancer, only one of the 691 gallstone patients followed in this study was found eventually to have an incidental carcinoma at operation, and further data are required to clarify this issue. Recent Swedish population postcholecystectomy follow-up data after a mean of 15 years revealed a weak increased risk of oesophageal adenocarcinoma with a standardised incidence ratio of 1.29. This is hypothesised to be due to increased oesophageal bile acid exposure.29 Further randomised data have revealed that surgery remains the best treatment for symptomatic gallstones, but conservative management may in selected circumstances be used in the elderly.30 In the early 1970s there was great interest in the use of dissolution agents, principally chenodeoxycholic acid (CDCA), in the treatment of gallstones.31 Prerequisites for attempting dissolution therapy were a functioning gallbladder, multiple small stones (which have a greater total surface area for contact with the dissolution agent rather than a smaller number of larger stones) and radiolucency (indicative of pure cholesterol stones without a calcium or pigment matrix to impede dissolution). Success was slow to be achieved in most subjects, usually taking 6–12 months as judged by the disappearance of stones on ultrasound. Side-effects of treatment included abdominal cramps, diarrhoea and occasional LFT abnormalities. Ursodeoxycholate (UDCA) has been shown to be equally effective as CDCA in dissolving gallstones. In patients administered dissolution agents, O’Donnell and Heaton32 found that recurrence rates increased rapidly in the first few years, with rates of 13% at 1 year, 31% at 3 years, 43% at 4 years and 49% at 11 years. Although recurrent stones were readily redissolved, they generally recurred when therapy ceased. Success with lithotripsy for renal stones led to the use of the same techniques for gallbladder stones. Early lithotripters, with immersion in large water baths, were soon succeeded by smaller devices with a limited area of contact via a water-filled cushion. Biliary anatomy, however, did not lend itself to a repeat of the success observed with renal stones. The tidal flow of bile into and out of the gallbladder, along with the presence of multiple gallstones, were factors that contributed to the failure of the technique. Ahmed et al.33 reported that 45% of patients undergoing lithotripsy required subsequent cholecystectomy. Lithotripsy has therefore been retained only for the management of ductal stones resistant to endoscopic removal.34 The operative mortality of open cholecystectomy for cholelithiasis had fallen in the years before the introduction of laparoscopic surgery, with many series reporting operative mortality rates of less than 1%.35 Common duct exploration was regarded as increasing the risk of open cholecystectomy by four- to eight-fold.36 In a comparative study between a North American and a European centre, 12–14% of patients developed complications, and the bile duct was explored in 8.6% of the patients in Toronto as opposed to 17.9% in Geneva, the incidences of positive exploration being 61% and 73%, respectively. Factors increasing the risk of postoperative mortality were advancing age, acute admission, admission to hospital within 3 months of the index admission, and the number of discharge diagnoses.36 Only 18% of postoperative deaths in this study were related to the gallstone disease or the surgery, with underlying cardiovascular or respiratory disease contributing to 48% of deaths. There has been considerable uncertainty regarding the true incidence of bile duct injury at open cholecystectomy, and the surveys available cite figures of one injury per 300–1000 operations.37 At cholecystectomy, injury results from imprecise dissection and inadequate demonstration of the anatomical structures.38 Although some patients do have anatomical anomalies or pathological changes that increase the risk of duct injury, it is noteworthy that in the extensive Swedish review, the patients most at risk appeared to be young, slim females who had not undergone previous surgery.37 In a detailed analysis of a consecutive group of patients undergoing cholecystectomy for presumed biliary pain in a District General Hospital between 1980 and 1985, Bates et al.39 compared the outcome of an age- and sex-matched control group of surgical patients without gallstone disease. Flatulent dyspepsia was more frequent in gallstone patients but operation markedly reduced these symptoms to an incidence almost identical to that of the control group. However, within 1 year of cholecystectomy, no less than 34% of patients still suffered some abdominal pain and none of the 35 patients referred back to hospital for investigation had evidence of retained ductal stones. Multivariate analysis showed that preoperative flatulence and long durations of attacks of pain were risk factors for postoperative dissatisfaction. There have been few controlled trials; of those that have been performed, one showed laparoscopic cholecystectomy to be superior and the other showed mini-laparotomy cholecystectomy as superior.40,41 The most recent randomised trial has again confirmed a smoother convalescence for laparoscopic cholecystectomy, although operating times remained longer.42 Symptomatic gallstones: The laparoscopic procedure can be offered to all patients with symptomatic gallstones, providing their cardiorespiratory status does not preclude laparoscopy. Of all patients presenting for operation, 95% can be completed successfully by laparoscopic means. Obesity, acute inflammation, adhesions and previous abdominal surgery do not usually prevent a laparoscopic cholecystectomy, but may require some adaptations of technique to complete the procedure.43–51 Techniques of laparoscopic cholecystectomy have been well described previously,43,44 including cases performed under regional anaesthesia in patients with chronic pulmonary disease.45 Laparoscopic cholecystectomy has been widely reported in pregnancy46 and in patients with cirrhosis.47 In a substantial audit of seven European centres,43,44 96% of procedures were completed successfully in the 1236 patients and only four bile duct injuries were reported. There were no postoperative deaths, median hospital stay was 3 days and the median return to normal activities was only 11 days. Acute cholecystitis: Fears that laparoscopic cholecystectomy in the management of acute cholecystitis could carry an unacceptable risk of disseminating infection or of perpetrating an injury to the bile duct appear unfounded.51 Several large series report success and safety with this procedure, although the incidence of bile duct injury and conversion to open operation remain slightly higher.52 In difficult cases, improvement in the exposure of Calot’s triangle may require additional or different positioning of the laparoscopic cannulae, the use of oblique viewing telescopes and placement of endoscopic retractors. Decompression of a distended or inflamed gallbladder may also improve access. Complications: The mortality rate in a good-risk patient undergoing elective operation is less than 1% and operative risks usually arise from comorbid conditions. The laparoscopic technique is associated with lower wound infection rates than open surgery.53 Furthermore, a recent meta-analysis has shown that antibiotic prophylaxis is not warranted in low-risk patients undergoing laparoscopic cholecystectomy.54 Day-case laparoscopic cholecystectomy: Worldwide, laparoscopic cholecystectomy is being performed in the day-case setting with good preoperative patient selection, improved techniques, and improved postoperative control of pain, nausea and vomiting.55 Needlescopic cholecystectomy: This technique has been described using 2- and 3-mm instruments and a 3-mm laparoscope. A randomised trial has shown less pain and smaller scars when this technique was used in patients with chronic cholecystitis.56 Evolution of technical aspects of multiport exposure, decreasing port sizes and instrumentation continues. There is currently no evidence of a benefit for single-incision laparoscopic port techniques,57 with impaired ergonomic performance and probable increased incisional hernia rate. Bile duct injury: Anxieties regarding an increased incidence of bile duct injury with the introduction of laparoscopic cholecystectomy have not been substantiated by multicentre studies from Europe48 and the USA,49 with a reported incidence of injury to the CBD of 1 in 200–300 cases. In a study in the West of Scotland, a prospective audit of laparoscopic cholecystectomy was undertaken.58 A total of 5913 laparoscopic cholecystectomies were undertaken by 48 surgeons, and 37 laparoscopic bile duct injuries were reported. Major bile duct injuries were defined as those where laceration to more than 25% of the bile duct diameter occurred, where the common hepatic duct or CBD was transected, or in those instances when a bile duct stricture developed in the postoperative period. Of the 37 injuries, 20 were classified in this way, giving an incidence of 0.3%. Delayed identification of bile duct injury occurred in 19 patients and, although it was noted by the author that cholangiography did not play a part in the identification of bile duct injuries, it was noteworthy that imaging was used in only 8.8% of all laparoscopic procedures. During the course of this 5-year study, the annual incidence of bile duct injury peaked at 0.8% in the third year but had fallen to 0.4% in the final year of the audit. A meta-analysis of more than 100 000 cases reported an injury rate of 0.5%.59 Archer et al. emphasised the importance of supervised surgical training to allow attenuation of the trainee surgeon’s learning curve by the experience of his/her proctoring surgeon. The importance of cholangiography in the early detection of bile duct injury was also emphasised.60 Way et al. analysed bile duct injuries from a cognitive psychological perspective and concluded that errors that led to bile duct injury stemmed from anatomical misperceptions as opposed to errors of skill or judgment (Fig. 10.3). This analysis concluded with a list of rules to help prevent injuries.61 Figure 10.3 The ‘classical’ laparoscopic bile duct injury. (a) The common duct is misidentified as the cystic duct and is doubly clipped. (b) The common duct is then divided. (c) The gallbladder is retracted to the right, stretching the common hepatic duct and placing it in contact with the gallbladder. This is identified as an accessory duct and double clipped. (d) A high transection of the common hepatic duct results in the excision of most of the extrahepatic biliary tree.
Gallstones
Introduction
Composition, formation and risk factors
Presentation
Choledocholithiasis
Investigation
Blood tests
Ultrasonography
Endoscopic ultrasound (EUS)
Computed tomography (CT)
Magnetic resonance cholangiopancreatography (MRCP)
Endoscopic retrograde cholangiopancreatography (ERCP)
Management of gallbladder stones
Non-operative treatments for gallstones
Lithotripsy
Operative treatment of gallbladder stones
Mini-laparotomy cholecystectomy
Laparoscopic cholecystectomy
Gallstones